

A hoof wall infection occurs when pathogens establish themselves within the hoof wall and proliferate, causing a breakdown of the wall structure. This may present as cracks that are crumbling on their margins, a general breakdown of horn quality or bulging of the hoof wall itself. From the solear surface, they may be seen as a distortion to the wall and white line, with cavities present that are not seen when the foot is weight bearing. The cavities may appear between hoof care visits and can spread rapidly in a few weeks in shod and unshod hooves. These cavities will be filled with a crumbling, pungent mass, which is the remains of the digested horn and can occur in any area around the white line. On their own, these infections do not involve the sensitive tissues, but they may be an additional complication to either a complicated hoof crack or where an existing horn disruption (eg from an abscess or previous trauma) is growing.
Hoof wall infections can present issues for the farrier when maintaining the shod foot (ie difficulty nailing or frequent shoe loss) or may create cavities that pack with dirt and create lameness as a result of pressure in the unshod foot (Stashak, 2002; 2006; Duff, 2015). If the hoof wall is significantly damaged, the connection between the stratum medium and stratum internum can fail, resulting in reduced strength for the laminar connection and ultimately destabilising the distal phalanx (mechanical laminitis) (Stoltz, 2018). To deal with these infections, the cause must be established so that the correct treatment approach can be applied.
Anatomy
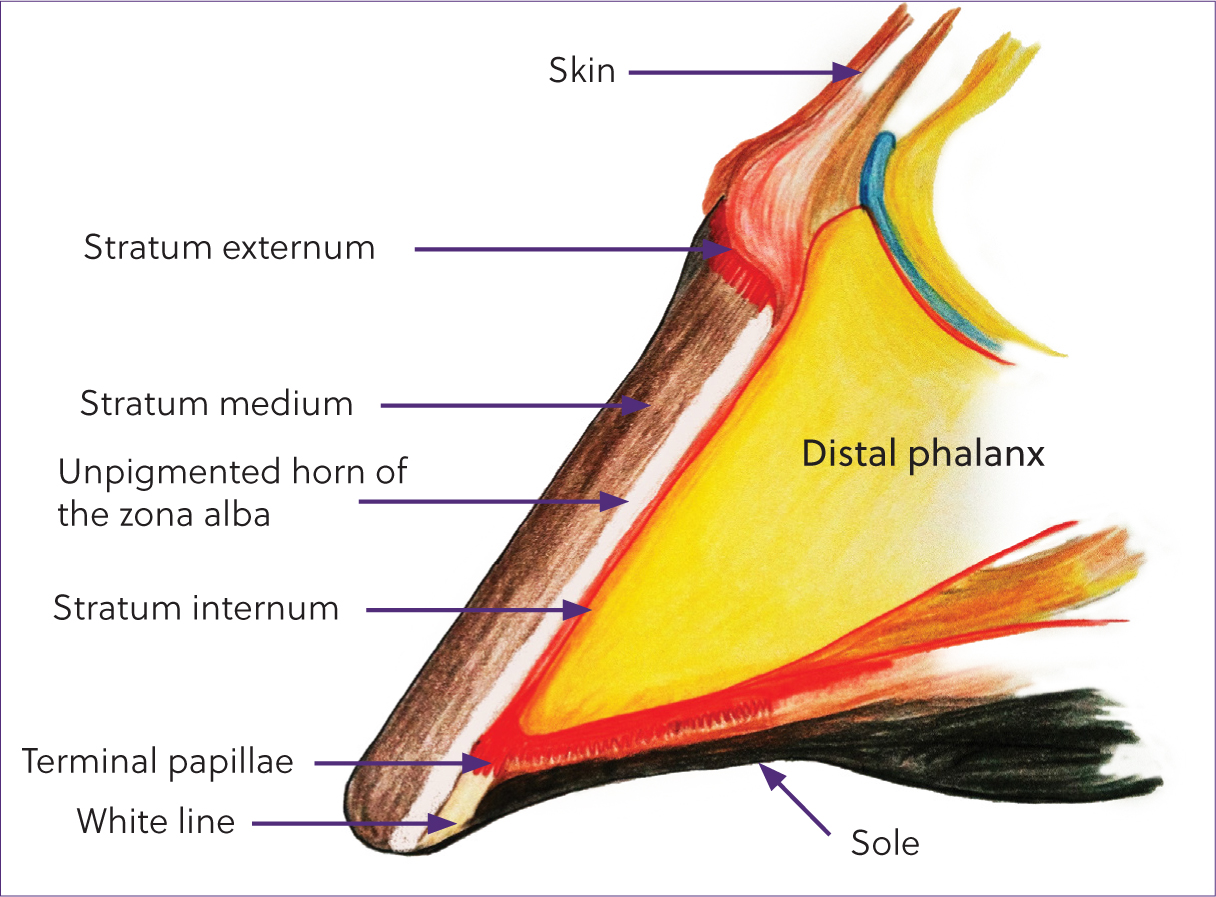
The hoof wall consists of three layers of horn (Pollitt, 1998; Reilly, 1998):
When observing the hoof from the solear surface, the interdigitation of the wall and the sole is denoted by the white line. This portion of horn is produced by the terminal papillae on the distal border of the distal phalanx (Figure 1).
The tubular horn found in the stratum medium is made of of hard keratin cells. These cells contain long-chain fibrous protein molecules (desmosomes), held together by disulphide bonds between the amino acids methionine and cysteine. Methionine and cysteine contain sulphur, which is required in the final stages of keratinisation, allowing the horn to harden fully as the cells die. Areas of horn such as the frog and the white line have fewer horn tubules, and less disulphide bonds. Therefore, they are not as strong; however, they have a higher number of lipids and sulphydryl groups (proteins containing sulphur) which provide elasticity to those areas (Pollitt, 1998). The horn tubules are found in four distinct layers of density within the depth of the hoof wall. The abaxial layer has the highest density of tubules and less density in each subsequent layer (Figures 2and3). This configuration of tubules means that the abaxial layer of the stratum medium is the hardest and most rigid, and the horn gets softer and more flexible deeper into the hoof (Reilly, 1998). This graduation of horn hardness and flexibility allows stress to be smoothly transferred across the wall, onto the lamellae and then the skeleton. Intertubular horn is found between the tubules, which is produced from basal cells on the stratum germinativum (basal layer), between the coronary papillae.
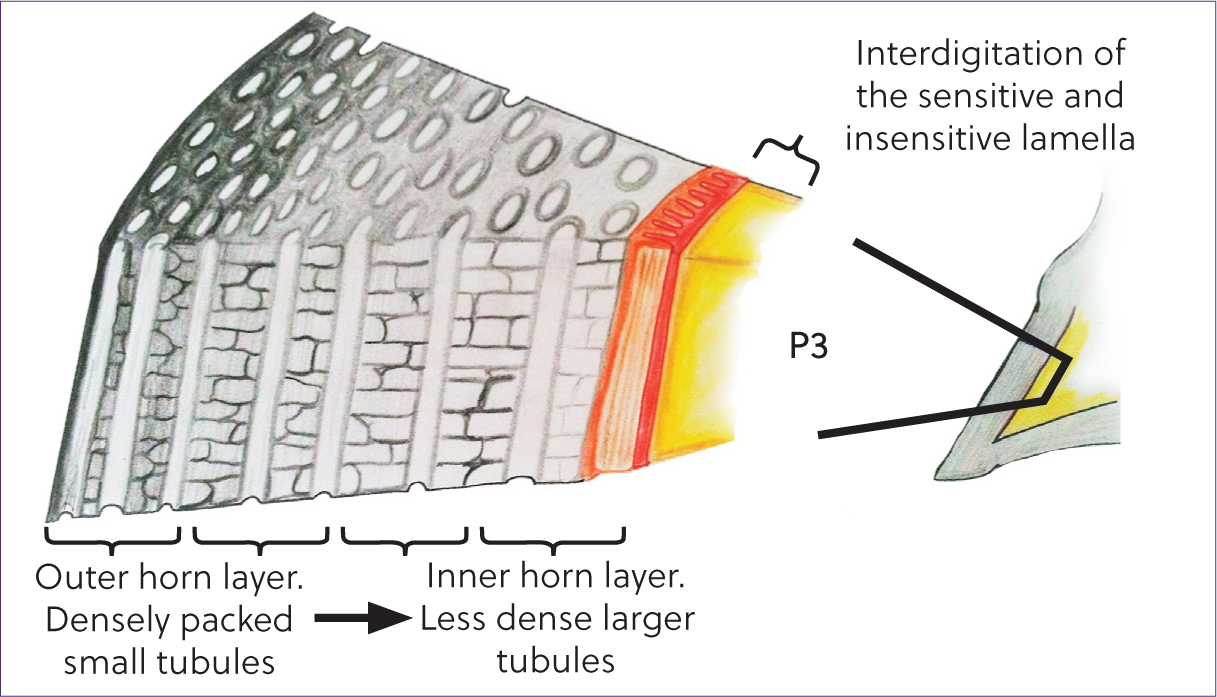
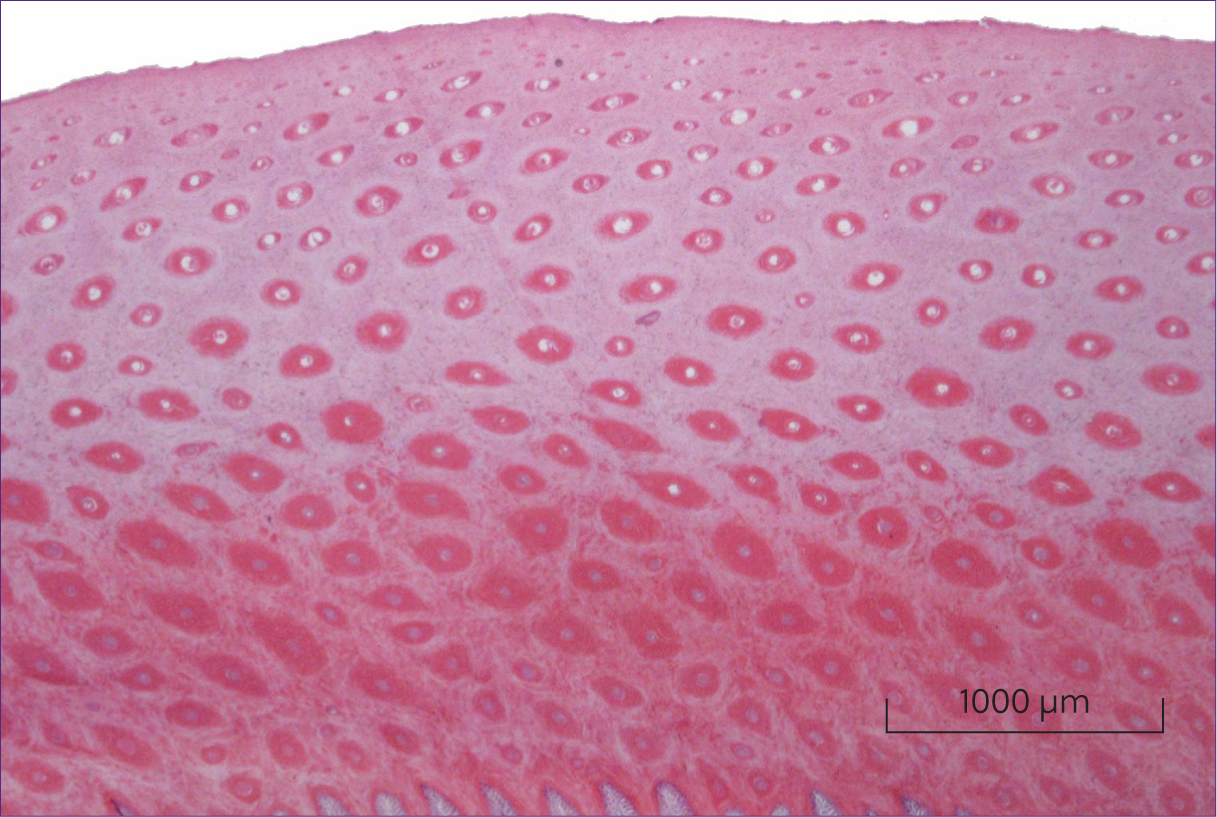
The horn tubules are solid on the more superficial layers of the wall but become more porous as they get deeper in the wall – starting in the middle of the stratum medium, the tubules are sectioned with air pockets around them which increase in density towards the edges of the stratum medium (Mahrous et al, 2023). The cells of the intertubular horn are produced at 90 degrees to the direction of the horn tubules, creating a matrix of continually hardening keratin around the tubules (Goodman, 2008). The structure of the wall and the greater availability of keratin and sulphur within the innermost layers of the stratum medium make this area the most viable location for fungal and bacterial proliferation.
Pathogenesis
There have been many studies looking at the different opportunistic bacterial and fungal species found in infected hoof walls (Turner, 1997; Kuwano, 1998; Kempson, 2004; O'Grady, 2021). There is agreement that the main fungal species found are the genus Scedosporium, which are a known soil fungus found worldwide. Scedosporium apiospermum or Pseudallexheria boydii, as the teleomorph of S. apiospennum, was isolated in cases of onychomycosis when looked at as a part of white line disease (Kuwano, 1998). There are also numerous different bacteria found in affected hooves (Kempson, 2006), where aetiology is unknown (Turner, 1997; Loving, 2022).
A hoof wall infection is keratolytic (causing disintegration of keratin) and is characterised by the damage and the subsequent separation of the stratum medium from the stratum internum. The pioneer organisms are sulphur-reducing bacteria which will cause destruction of the sulphur bonds between the keratin molecules (Kempson, 2006). The horn degradation is furthered by opportunistic keratinophilic species of fungi and bacteria. These organisms digest the elements of keratin, leaving the wall weakened or absent depending on the severity of the condition (Moyer, 2003).
Classification
Hoof wall infections have been given several different names over the last 200 years (eg white line disease, seedy toe, hollow wall and sometimes onychomycosis). These terms are used interchangeably, causing confusion about the mechanisms of the disease and potentially the relevant treatment. The term ‘keratolytic disease of the zona alba’ was first used by Curtis (2018) and is the first term to accurately describe the condition, therefore helping to remove confusion in communication between veterinary professionals and the horse owner.
Keratolytic disease of the zona alba is an invasion of pathogens into the inner layers of the hoof wall. Anaerobic bacteria and keratinophilic fungi cause separation between the stratum medium and stratum internum. The infection occurs in two distinct scenarios (Table 1), and this must be established before treatment can be successful as each require a different treatment method (Logie, 2015).
| Type 1: structural keratinolytic disease of the zona alba | Type 2: systemic keratinolytic disease of the zona alba |
|---|---|
| Where an insult or weakness occurs in the hoof, through a fundamentally isolated mechanical cause (eg cracks, unbalanced loading or incorrect hoof balance) | Environmental or systemic cause. Generally occurs in hooves showing inferior horn production and/or structure, with brittle outer layers of horn and/or signs of blackening around the nail holes or around the white line in general. Horses may have poor shoe retention or be lame, footsore and/or have chronic laminitis |
Logie (2017) carried out a study to find a treatment method that would prevent reinfection in areas of structural keratolytic disease of the zona alba (type 1), thereby reducing the chance of it becoming a chronic destructive condition and giving the farrier the ability to recover feet to full strength. Previous treatment relied on clean, dry conditions with good continuous management, and even that was not reliable for recovery.
Treatment method for type 1 cases
Trim the hoof to ensure good hoof balance, which encourages a level foot landing and equal joint loading. Debride the infected area until the visible extent of the infection is exposed and only solid horn is left. Prepare the resected area for filling by creating ‘keys’ for the thermoplastic to lock into (Figure 4). When using imprint granules, as the soft plastic is removed from the water, it should be dipped into copper sulphate powder, so that it creates a layer over the whole debrided area and up the edges of the hoof when applied. The plastic should then be applied and moulded to the foot and onto the sole. While the plastic is still soft, nail the shoe on. Put the foot down while the plastic is still soft so that no sole pressure is created once the plastic hardens. Finish off the clenches. Cool the patch with freezer spray to harden it, then seal with acrylic glue (Figure 5). To reduce the risk of infection or abscesses, do not fill any sensitive tissues that are present, until these areas have keratinised and become unresponsive to direct pressure. This method allows hoof capsule integrity to be retained; in large areas, an appropriate bar shoe is advisable for additional stability. The method should be repeated at each shoeing until the area has grown out.


Study design, materials and methods
This study used three different topical treatments under one type of filler against a control of the accepted treatment of debridement and owner controlled management. The study compared a treatment group of 19 hooves with visible areas of structural seedy toe >10 mm2. All horses were in similar management, and primarily on grass turn out.
All horses were shod by the author, at an interval suitable to their hoof growth and workload. At each subsequent shoeing, the area was measured and treated as per their allotted group. All owners had agreed to the treatments, signed a consent form and the data were kept securely to maintain confidentiality.
Hypotheses
The hypotheses were that a previously infected area, free from bacteria and fungi, could be filled and reinfection prevented if a topical dressing was applied under the patch, and that treated feet would return towards a solid, infection-free state faster than the control feet. For the statistical analysis, the null hypothesis was that there would be no difference between the groups.
Treatment groups
The hoof was trimmed and then debrided until the visible extent of the disease was exposed. The area was then photographed, measured, medicated and filled. Measurements were taken from the coronary hairline to the highest point of the debrided area (in line with the laminae), the widest point of the debrided area (at the base) and the height of the debrided area from the ground surface (in line with the laminae). The area the horse was stood on was always hard and swept clean. Initial treatment consisted of mechanical removal of affected horn using disinfected farrier tools, then the resected area was prepared for filling by creating ‘keys’ for the thermoplastic to lock into and treated with the randomly chosen product for that horse (Box 1). Once treated, the cavity was repaired in a prescribed method with thermoplastic, the shoe was nailed on, finished off, the patch was cooled to harden it then sealed with acrylic glue. The shod foot was loaded before the plastic was hardened, to help prevent sole pressure. To reduce the risk of infection or abscesses, the area was not filled until any sensitive areas had keratinised and become unresponsive to direct pressure. The type of filler used was chosen as it was moisture tolerant, non-exothermic and easy to remove which was necessary at each shoeing. Exothermic materials can cause problems if the resected area is close to sensitive tissue and may also react with the topical treatments (Curtis, 2006). At each subsequent visit, the presence of visible infection was recorded, and the size of the area resected was measured.
Welfare precautions in the treatment groups
If the hoof wall in the infection area of any foot was noted to have deteriorated after two consecutive treatments or no significant progress was seen after four treatments, then the treatment method was changed to prevent potential harm occurring to the horse through a further loss of hoof wall. The overall management for the treatment groups was not altered in any way during treatment.
Control group
The control group was identified as having hooves affected by structural seedy toe and were treated purely by debridement and exposure of the infected area. The affected areas of the feet were measured as per the treatment group and not medicated at the time or filled with a repair material. The owners of these horses were asked to keep the feet clean and dry between visits and treat daily with whichever over-the-counter topical dressing they had access to. The owners were not asked to use the same treatment as used in the other groups as the purpose was to replicate the current treatment methods, which tend to be those available from the saddlery supplies. Such treatments were not considered to be effective or long lasting enough to use under the patches in the other groups. One owner changed the management of the horse to prolonged stabling during treatment.
Study data
The summary of the group data is shown in Table 2. The start and finish area of each horse is shown in Table 3.
| Group | Number of feet | Initial area infected (mm2) (range) | Days treated (range) | Number of feet returned to solid | Feet moved from another group | Feet moved to other group | Feet with ongoing treatment at end of study |
|---|---|---|---|---|---|---|---|
| Control | 5 | 150–1400 | 119–282 | 0 | 0 | 2 | 5 |
| Iodine solution | 4 | 96–434 | 168–282 | 3 | 0 | 0 | 0 (1 sold) |
| SD115 | 4 | 176–875 | 55–323 | 1 | 1 | 3 | 0 |
| CuSO4 powder | 6 | 294.5–1250 | 77–288 | 4 | 4 | 0 | 2 |
| Group | Horse | Start area (mm2) | Finish area (mm2) |
|---|---|---|---|
| Control | 7 | 475 | 295 |
| Control | 12 | 150 | 370 |
| Control | 14 | 350 | 338 |
| Control | 15 | 240 | 240 |
| Control | 16 | 1400 | 630 |
| CuSO4 | 4 | 323 | 0 |
| CuSO4 | 11 | 1250 | 0 |
| CuSO4 | 12C | 391 | 128 |
| CuSO4 | 5B | 805 | 0 |
| CuSO4 | 6B | 350 | 348 |
| CuSO4 | 7B | 295 | 0 |
| Iodine | 1 | 434 | 0 |
| Iodine | 2 | 350 | 0 |
| Iodine | 3 | 313 | 0 |
| Iodine | 9 | 96 | 96 |
| SD115 | 5 | 875 | 805 |
| SD115 | 6 | 176 | 350 |
| SD115 | 8 | 220 | 0 |
| SD115 | 12B | 370 | 391 |
Results
Reinfection results
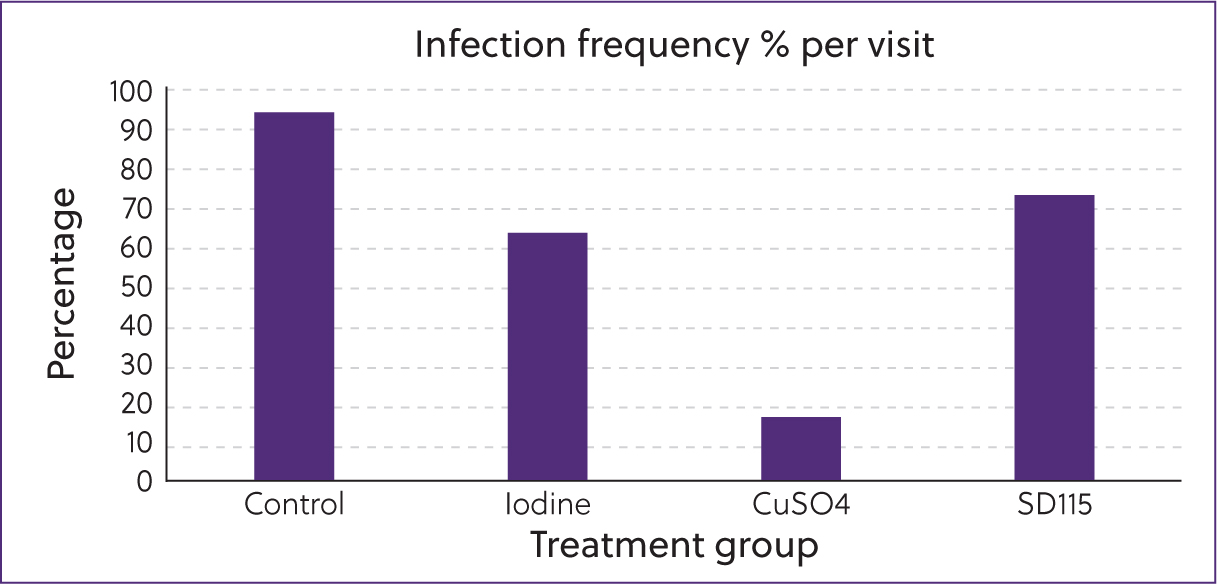
There were clear differences between the groups (Table 4), with the control group having the highest rate of reinfection, followed by the SD115 gel, the Iodine solution then the copper sulphate powder having the lowest rate of reinfection (Figure 6). The frequency of reinfection in each group was calculated by the number of occurrences of infection, divided by the number of visits and multiplied by 100 to give a percentage.
| Visit 1 | Visit 2 | Visit 3 | Visit 4 | Visit 5 | Visit 6 | Visit 7 | Visit 8 | Sum | |
|---|---|---|---|---|---|---|---|---|---|
| Days of treatment | 0 | 27–63 | 77–126 | 126–189 | 168–252 | 232–267 | 282–288 | 323 | |
| Control infected | 5 | 4 | 5 | 4 | 3 | 1 | 0 | 0 | 22 |
| Control non-infected | 0 | 1 | 0 | 1 | 0 | 0 | 1 | 0 | 3 |
| Iodine infected | 4 | 2 | 1 | 1 | 1 | 1 | 0 | 0 | 10 |
| Iodine non-infected | 0 | 2 | 3 | 3 | 2 | 0 | 1 | 1 | 12 |
| CuSO4 infected | 5 | 0 | 0 | 0 | 0 | 0 | 0 | 0 | 5 |
| CuSO4 non-infected | 1 | 6 | 6 | 4 | 4 | 2 | 1 | 0 | 24 |
| SD115 infected | 4 | 3 | 3 | 2 | 3 | 1 | 1 | 0 | 17 |
| SD115 non-infected | 0 | 1 | 1 | 1 | 0 | 1 | 1 | 0 | 5 |
Treatment options
Chi squared test results
The results were tested to P<0.05, and were also significant with P values at 0.001 and a Chi squared value of 32.94. The further tests showed that there is a significant difference between the groups. The partitions showed:
Hoof recovery results
Each horse has an individual hoof growth rate, and this is their maximum possible area reduction rate. This growth rate cannot be altered by a treatment applied to the distal border of the hoof wall. If visual infection is present and further debridement is required, the area reduction rate is slowed down. The graphs (Figures 6, 7and8) show the reduction in the area affected, over the time they were treated. The presence of visible infection is denoted by a black data point.
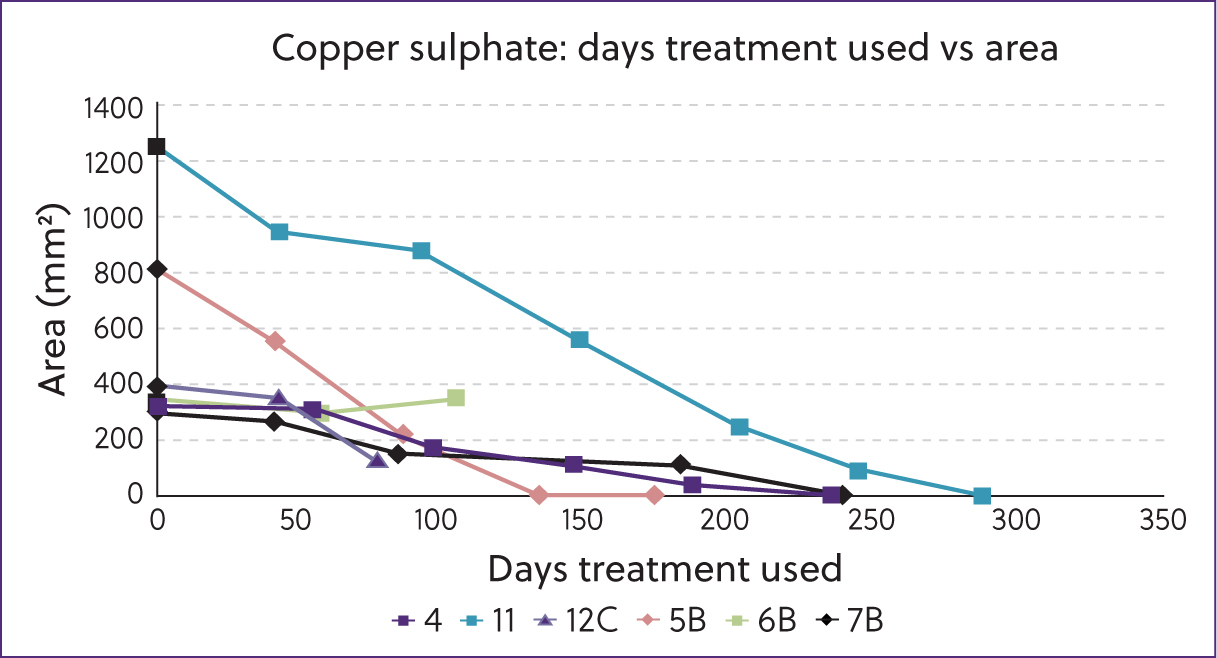
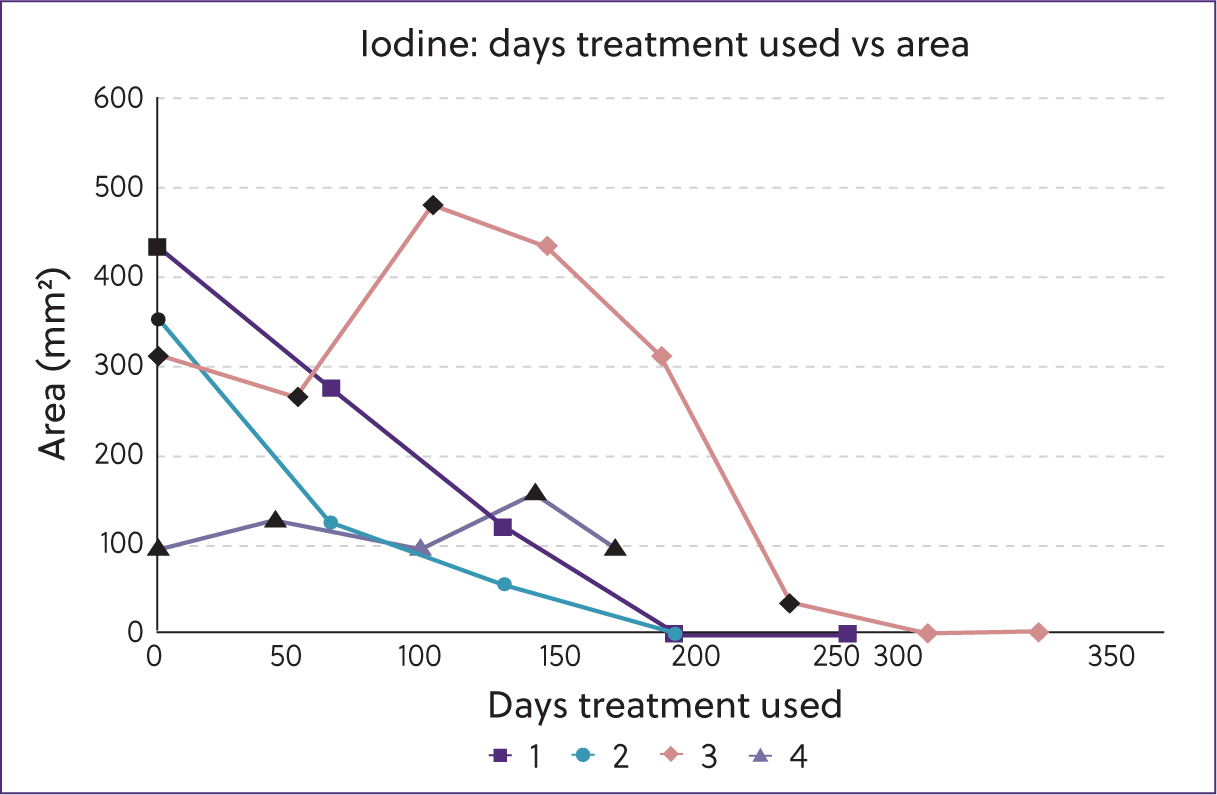
As the horses were all started at a separate time, and some were changed into a different treatment group, their data lines appear to stop mid-graph. This was because the study was completed before they had grown out, although their treatment continued. The results show a consistent level of improvement for the copper sulphate powder (Figure 7) and iodine solution groups (Figure 8).
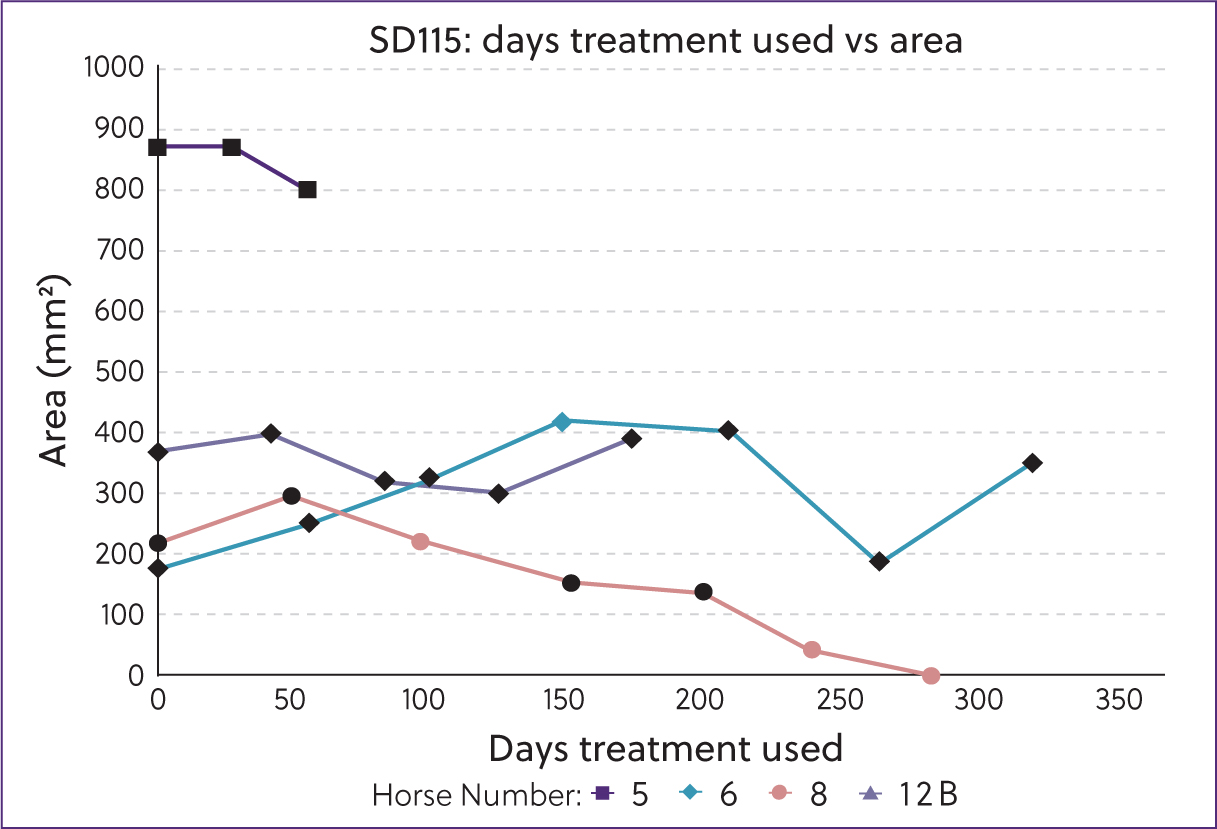
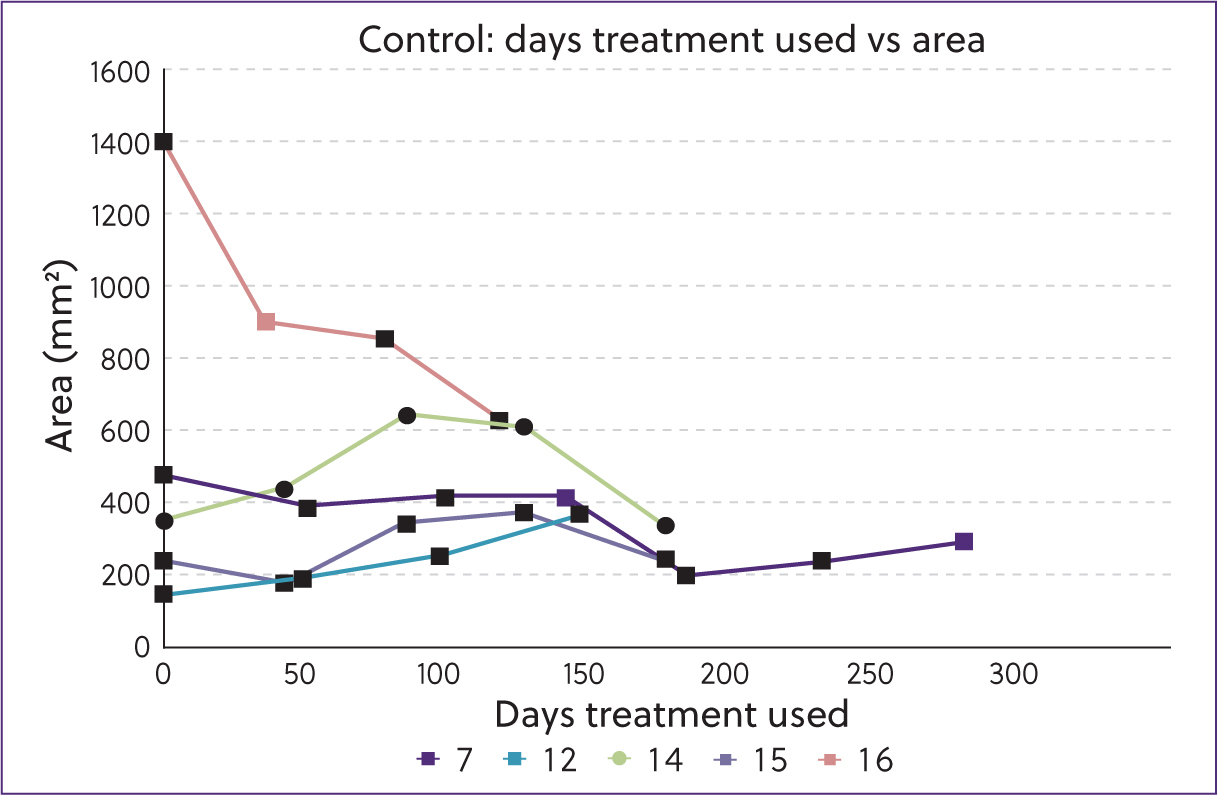
The SD115 group showed marginal change in the feet (Figure 9), and the control group showed that a majority of the feet had either an increase in the size of the debrided area or minimal reduction in area. This was because of the high occurrence of visible infection (Figure 10).
Summary of results
The results show that the frequency of reinfection was significantly different between the four groups (P<0.05); results were also still significant at P<0.001.
Chi squared partition testing showed that there was no difference between the SD115 and control groups (P>0.05). Therefore, it was not the application of the patch that was making the difference. Chi squared partition testing also showed that the application of copper sulphate or iodine solution significantly reduced the frequency of reinfection (P<0.05), allowing the hoof to re-grow and return to a solid structure.
The application of copper sulphate powder or iodine solution increased the rate at which the hoof could be returned to a solid state, although this was not statistically significant when observing the area reduction against the days of treatment.
Discussion
The study showed that the application of copper sulphate powder under the patch produced the fastest recovery in an individual case. The significant results showed that reinfection can be prevented between treatments, with an easy, cost-effective patching method that is already widely used within farriery. This method allows the farrier to control the treatment, and the owner is no longer required to change the horse's management. On a microscopic level, it has been shown that copper sulphate can damage horn cells (Kuwano, 1998). However, its use is less damaging to the hoof integrity than the infection, as far more horn cells are lost during debridement.
Anecdotally, farriers have successfully recovered infected hooves with this method, but using other filling methods (eg acrylics). The important factors when using this method are the use of medication that is active throughout the shoeing cycle and the use of a patch to minimise the risk of further contamination. Although the method used by Logie (2017) was successful in the shod horse, the unshod horse will need some addition to the patch to enable it to stay in the hoof. This has anecdotally been shown to be more effective than leaving the area open to reinfection.
Recorded changes in the environment, resulting in milder and wetter UK conditions, mean that more attention should be given to what may appear to be minor invasions on the bottom of the hoof. Proactive methods that are easy and inexpensive to apply and beneficial to overall hoof health should be encouraged. If minor infections are treated very early, they rarely get large enough to require debridement and patching. Further research is required into finding a treatment that is as effective as copper sulphate but safe to use near sensitive tissue, as the method cannot be used if sensitive tissues are exposed during the debridement process.
Conclusions
Type 1 keratolytic disease of the zona alba poses a risk to the strength and integrity of the hoof capsule. When it becomes extensive, it can cause lameness and a challenge to the farrier. If treated in a proactive method, even extensive areas of compromised hoof can be restored and protected. By using a topical treatment under a thermoplastic filler, the risk of reinfection is greatly reduced, speeding up the restoration time for the hoof capsule and removing the reliance on third party management. Copper sulphate powder was the most effective topical treatment to prevent reinfection between shoeing visits and does not require ongoing debridement of the hoof wall which prolongs the recovery time. A medicated patch is an easy-to-use method in cases where occurrence was unexpected. Other proactive treatments, such as a chlorine-dioxide foot soak, are less convenient for the farrier and medicated patches using antibiotics are not accessible to farriers or recommended, given the heightened awareness of antibiotic resistance. This is an easy, reliable, affordable and effective method of treatment for type 1 keratolytic disease of the zona alba.