

With the ongoing development of imaging techniques, veterinarians are able to gain more information about the cervical region of the horse. Cervical dysfunction refers to a range of issues affecting the cervical spine and surrounding tissues, which may lead to, for example, a restricted range of motion, pain, an asymmetric gait pattern, neurological deficits, behavioral changes and/or muscle atrophy. With this abundance of data, veterinarians must be sure not to lose sight of the horse and to determine what clinical relevance these findings may have. Good clinical examination in combination with knowledge of functional anatomy and biomechanics are required while research to allow a more evidence-based approach is ongoing.
History
The basis of every examination is a good history. Indications of neck problems in the owner's story may include an incident of trauma (eg a fall after a fence), but also functional limitations and pain complaints leading to, for example, abnormal pressure on the bit, lameness, headshaking and behavioural problems. Owner complaints may include a difference in lateral bending to the left compared to the right, increased rein tension, a horse that does not want to make contact with the bit or has difficulty with a certain position of the neck. The horse may hold the head and neck rotated or in extension. In terms of behaviour, the horse may hop forwards during the transition from walk to trot, be reluctant to move forward, may stop, rear or show flight behaviour. A horse may panic when forced into a certain head and neck position or, for example, when changing lateral bending from left to right or vice versa. Horses with neck problems are often easily irritable, sensitive and sometimes anxious. In addition, there may be a shortened protraction and/or irregularity in the foreleg, frequent stumbling or loss of balance.
Static observation
The clinical examination begins with a static observation. The entire body is assessed, as neck problems can occur secondary to other pathology. Does the horse look bright and alert, is it introverted, does it show signs of pain (ie pain face) or is it panicky? Horses with cervical pain may become easily stressed. Given the segmental innervation, the development of the musculature around the topline is often a good indicator to assess which region is causing problems (Grönberg, 2014). In addition, spinal alignment can be evaluated. Does the spine show the usual curve or do some regions show more extension or flexion than usual? The horse may be rotated in the neck or show more lateral bending to one side. Spinal alignment refers to how the vertebrae line up with each other. In neutral position, the cervical spine should show an S curve. Behind the withers, the back shows thoracic lordosis and kyphosis at the lumbar region. This is the normal alignment in the sagittal plane, and Haussler (2003) defined the normal range of motion for each segment of the spine. The horse should not show scoliosis in the coronal plane nor rotation in the transverse plane in a neutral position. When evaluating neuromuscular function, the horse's ability to ventrally stabilise the spine is assessed. Gravity on the mass of the abdomen in combination with the ground reaction forces on the legs will pull the spine in extension. The bow and string principle to counteract this was first described by Slijper (1946). Slijper (1946) suggested the analogy of an elastic bow (pelvis and body-axis of the trunk) bent in the dorsal direction (ventral concave) by a string (sternum, abdominal muscles, linea alba, extrinsic muscles of the legs). To assess if the horse is able to use this bow and string principle (counteract the forces of gravity by ventral line engagement), one can evaluate the amount of flexion in the spine, the location of the ventral border of the abdomen, the distance of the dorsal border of the scapula to the withers and the position of the legs. The stance and limbs are checked, as well as any signs of neurological or neuropathological signs. Because the spine contains the spinal cord and the nerve roots, spinal pathology may lead to neurological deficits, eg as a result of compression of the spinal cord or impingement of the nerve roots.
General palpation
During general palpation the whole body is palpated, looking for abnormalities in muscle tone (increased or decreased), increased temperature, sensitivity or pain, swelling or other deviations. These changes can occur generally, regionally (eg the cervical region), segmentally (eg the region innervated by one segmental nerve) or focally. By working systematically from mandible to tail, no regions of the spine are missed. In horses with cervical dysfunction, the rhomboid and brachiocephalic muscles often show hypertonicity. Anecdotally, compensatory hypertonicity of the muscles of the cranial, cervical and thoracic regions can be found in cases with caudal cervical pathology.
Motion evaluation
Motion evaluation provides insight into the mobility and/or range of motion, quality of motion, pain and end feel (Figure 1). ‘End feel’ describes the quality of resistance felt by an examiner at the end of a passive movement of a joint. The cervical spine is initially tested with general lateral bending to the left and right. This can be performed by gently leading the horse via the headcollar. A carrot test is less reliable, as it invites the horse to throw its head and neck to one side, leading to compensation patterns such as rotation to reach the goal. General lateral bending should be requested from the horse in a guided and controlled way, so that the quality of movement and the amount of compensation are much easier to assess. After the general tests, all segments are tested individually. For the cervical region this starts with flexion, extension and lateral bending of the occiput–C1 joints. All tests incorporate the full range motion to come to an end feel. This end feel should be elastic and smooth without any signs of pain. Signs of pain may include increasing tension in muscles during testing, muscle fasciculations, pinning of the ears, avoiding pressure of the testing hand, stepping away and even biting if not tested subtly. Stiffness or crepitus may be evident. Rotation of C1–2 is tested, after which C2 until T1 articular process joints are tested for lateral bending. This is followed by testing the C2–T1 articular process joints for flexion and extension. Motion evaluation tests are continued for the whole spine as well as the head, limbs and tail to exclude other primary causes for cervical dysfunction, eg temporomandibular joint pain, other pathology causing limb lameness or back pain.

Specific palpation
With specific palpation, locations of interest are palpated in more detail. This could be anything from a local swelling (eg at the location of the cranial nuchal bursa) to the articular process joints and the attachment of the semispinalis tendons. Temperature is evaluated as well as the shape, texture, pain response and the presence of any oedema (Figure 2).

Dynamic examination
A horse can be evaluated in hand, at lunge or under saddle. Typical cervical dysfunction-related findings may include decreased cervical mobility, hopping when transitioning from walk to trot, cervical extension, decreased coordination, decreased (outer) front limb protraction, lameness, stumbling, cantering with an upward motion in the front quarters, rotation of the neck and so on. Signs of pain can be detected in both unridden and ridden horses (van Loon et al, 2021; Dyson, 2022), varying from facial expressions to stopping and rearing. The use of side reins during lunging and riding may further worsen symptoms. Sometimes, symptoms can be provoked by requesting a certain head and neck position. The horse may show a flight response, so it is very important to decide if the horse can be evaluated safely under saddle to reduce the risk of accidents.
Additional examinations
In many cases, clinical examination will pinpoint the location from which the pain originates, so diagnostic analgesia is usually unnecessary. However, diagnostic analgesia of the articular process joints, nerve roots and semispinalis tendon enthesis can be performed if further localisation is required. A magnetic motor evoked potentials test, transcranial magnetic stimulation or transcranial electrical stimulation may be used to evaluate the function of the spinal cord. In horses with ataxia, when a problem in the motor nervous system is suspected, the results of these tests may be indicative of decreased neural conduction. Electromyography can be performed when a neuropathy of skeletal muscles is suspected. Cerebrospinal fluid collection is an option when, for example, a bacterial or protozoal infection is suspected.
Diagnostic imaging
A list of differential diagnoses is formulated based on the findings of the clinical examination, and diagnostic imaging is used to investigate further. Besides radiography and ultrasonography, large-bore computed tomography examination is available in certain equine hospitals, enabling the evaluation of the head and full cervical spine up to T3–5, depending on the size of the horse. This provides a wide array of images and information. All imaging findings should be related to the findings during the clinical examination and the presenting complaint. A veterinarian needs to have excellent knowledge of functional anatomy and biomechanics to identify which findings are clinically relevant to the horse. Recently, an increasing number of research studies on cervical pathology have been published, helping determine the clinical importance of particular imaging findings. A comparative study of breed differences in anatomical configuration of the equine vertebral column showed morphological changes in the caudal cervical region, including including abnormal shape and/or transposition of (part) of the ventral lamina of C6 and rudimentary first rib(s), in 43% of warmblood horses, 6% of Shetland ponies and 0% of Konik ponies (Spoormakers et al, 2021). The clinical implications of these changes are debated – some studies indicate this finding may increase the odds of horses showing neck pain and ataxia (Beccati et al, 2020) whereas other studies found no relation with cervical dysfunction (Veraa et al, 2016).
Radiography
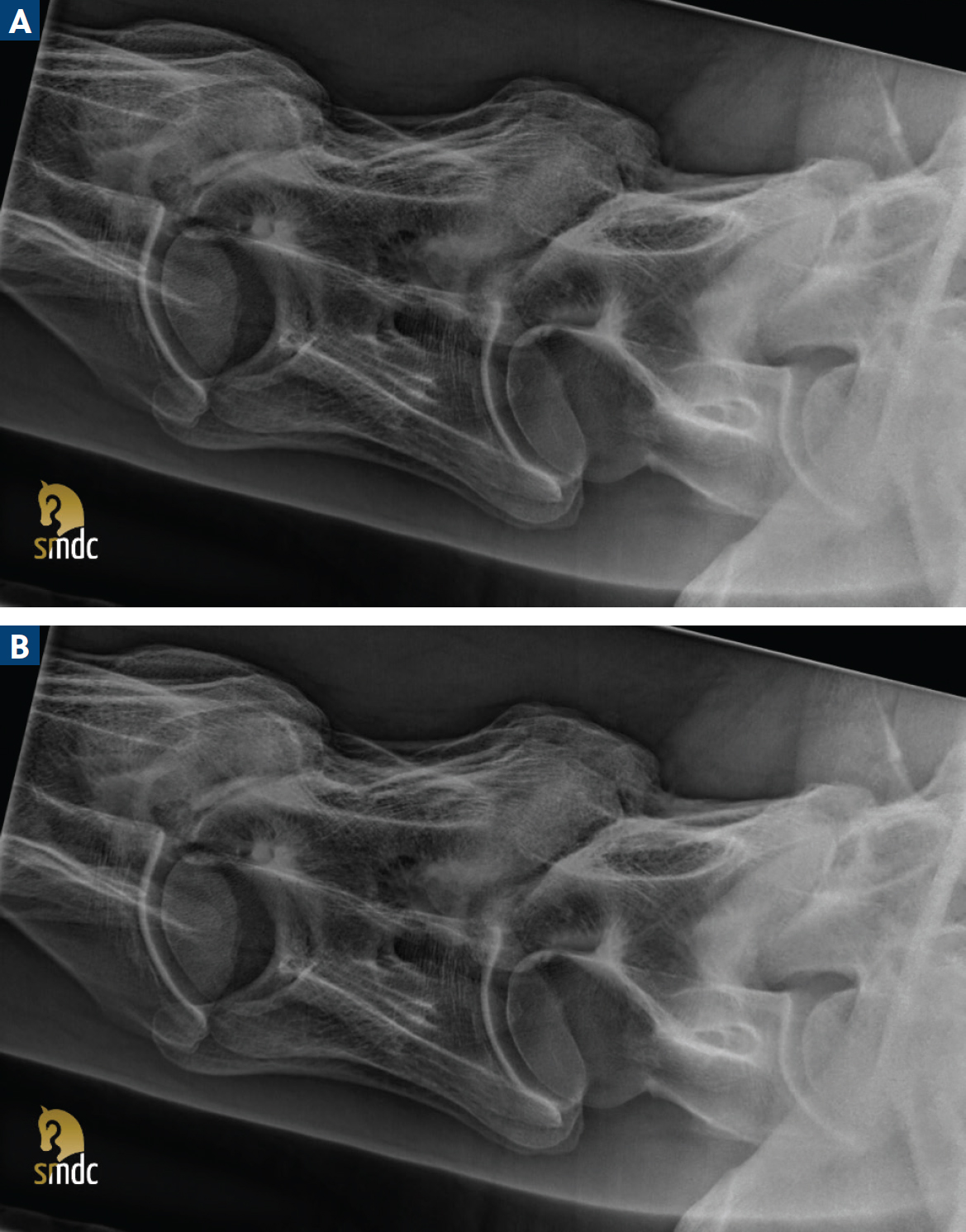
Radiography of the cervical spine is readily available, easy to perform and can be done in the sedated horse. Cervical radiography requires excellent positioning of the horse, collimation and good quality equipment (Figure 3). Neck position influences the commonly performed radiographic measurements (Beccati et al, 2018) and horses with cervical pain may be reluctant to keep a straight posture. The caudal cervical area, in particular, poses a challenge when taking radiographs, as the overlying shoulder regions increase the mass and therefore the scatter. Always work with the ALARA (as low as reasonably achievable) principle and step as far back as possible while wearing protective measures to decrease exposure. To correctly evaluate the images, the lateral and oblique images must be taken at exactly the correct angle and include the occiput and T1, as most pathology is located between C5 and T1 (Figure 4) (Rovel et al, 2021a). If the images are not straight or taken at the correct angle, then there is a risk of overinterpretation (eg abnormalities in articular process joint size and architecture) or under-interpre-tation (eg pathology located at the cervicothoracic junction). The first ribs may also be affected in the case of cervicothoracobrachial syndrome (Denoix, 2022). This syndrome includes all morphological variations in the caudal cervical and cranial thoracic region. This not only includes bony and joint-related changes, but also all other anatomical structures including muscles, arteries, veins and nerves.

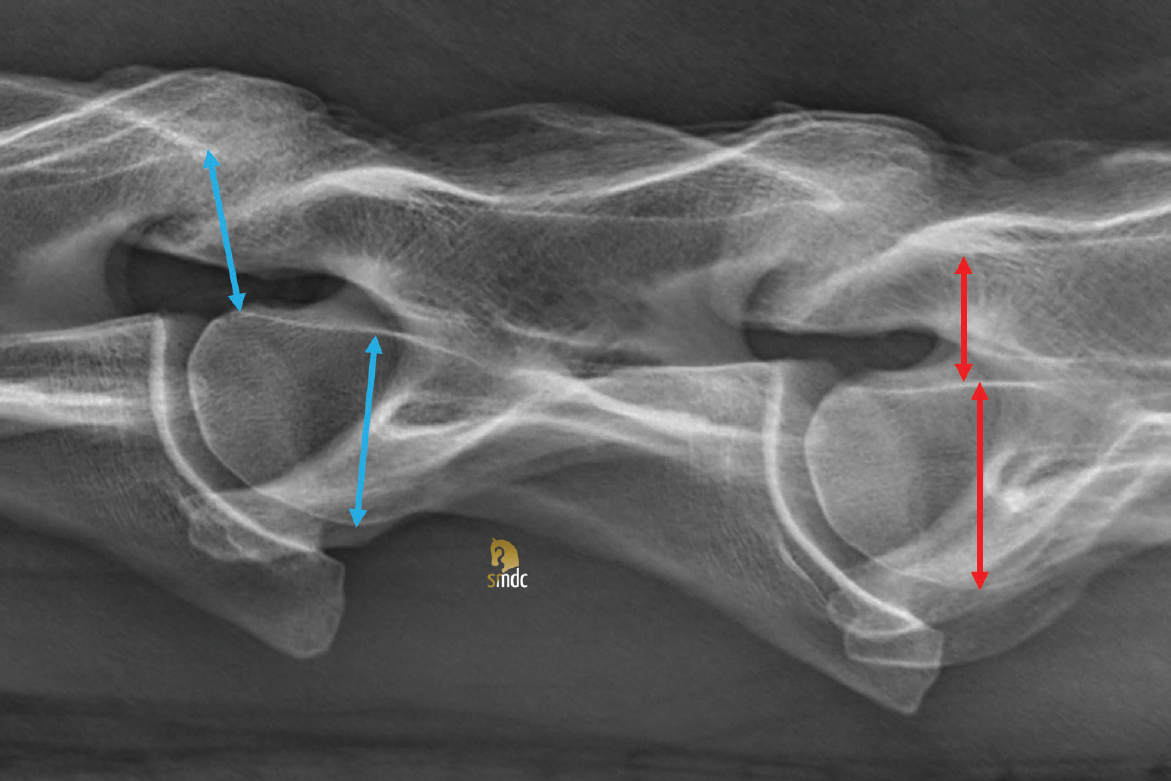
A radiographic grading system for cervical articular process joint osteoarthritis is not commonly used in practice, although some have been reported (Crijns and Broeckx, 2021). One study found a significant difference in grade for C5–6 and C6–7 articular process joints between horses with clinical signs and healthy horses (Koenig et al, 2020). Dressage horses were overrepresented in this study, and the interobserver repeatability was only moderate at 56% (Koenig et al, 2020). Inter- and intravertebral measurements (Figure 5) can be used to evaluate cervical vertebral malformation, and myelography with the cervical region in various positions (flexion, extension and neutral) can be useful in identifying sites of possible compression. In sports horses, the compression is often caused by articular process joint enlargement and/or synovitis or soft tissue swelling. On a lateral radiograph, inter- and intervertebral ratios can therefore be within normal limits even though the horse has compression of the spinal cord. Spinal alignment can also be evaluated by taking radiographs in various neck positions (Hahn et al, 2008; Hughes et al, 2014).
Ultrasonography
Ultrasonography is readily available, cheap when compared to other cervical imaging modalities and can easily be used on the yard without the implications of radiation safety (Figure 6). It is a valuable tool to evaluate soft tissue changes eg at the level of the semispinalis tendons, bursae, muscles and ligaments. However, it is also a very sensitive modality and can be used to evaluate periarticular changes of the articular process joints and diagnose changes when capsulitis, synovial effusion and/or synovitis are present (Berg et al, 2003; Denoix, 2009). It provides a practical way to evaluate the caudal cervical region as well as the first ribs and their surrounding structures in the field, if high-quality radiography is not available. Ultrasonography is also useful for taking guided spinal fluid samples and assessing improvement during rehabilitation, and it is essential for guided injections of articular process joints and other locations. Limitations include the evaluation of cervical stenosis, vertebral subluxation or nerve root impingement as the covering bone reflects the ultrasound waves (Denoix, 2022; 2024).

Computed tomography
Computed tomography is considered the gold standard for equine cervical imaging, as it provides high-resolution images that can distinguish between different types of tissue and produce threedimensional reconstructions. Contrast computed tomography (myelography) is useful to identify locations of spinal cord compression (Rovel, 2021b). Large-bore computed tomography equipment provides cross-sectional imaging of the cervical spine from the occiput to T5, even in large horses. In the standing horse, the head and cervical region up to C3 can be imaged (Figure 7). The rest of the cervical region and the cranial thoracic region can be imaged if the horse is placed under general anaesthesia.

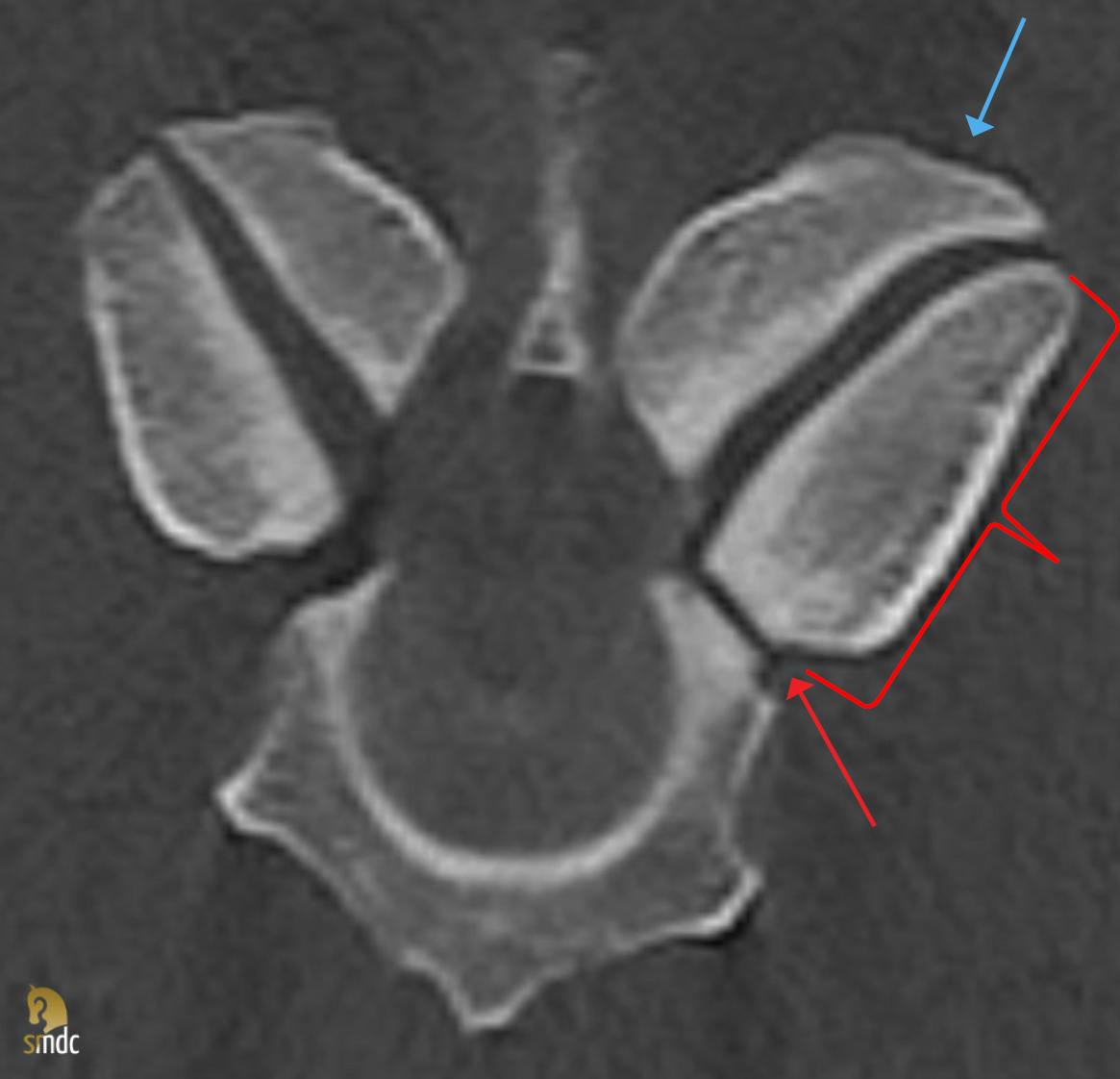
The most commonly found abnormality is narrowing of the intervertebral foramen (Figure 8) (80.2%), which is mostly frequently caused by enlarged and misshapen articular processes (Figure 8) (92.7%) (Rovel et al, 2021a). This is easily underdiagnosed on radiographs. Other frequent findings include degenerative changes (74.6%), periarticular osteolysis (57.7%), cyst-like lesions (35.2%) and fragments (29.6%) (Rovel et al, 2021a). Lindgren et al (2021) found pathology of the cervical vertebral column in 97.8% of observed cases, with 83% of cases showing evidence of articular process joint osteoarthritis. Impingement and compression of the spinal cord was found in 85% of cases, and 90% of pathology was diagnosed caudal to C5. Spinal cord compression was identified in 31 out of 51 (61%) horses with myelography in another study (Gough et al, 2020). Currently, multiple centres are collecting data to develop dual energy computed tomography. This technique may enable the detection of fluid within the bone in the future.
Magnetic resonance imaging
Unfortunately, magnetic resonance imaging examination of the (caudal cervical) region is currently impossible in a live horse, because of the size of the region. Studies are usually based on ex vivo images, but generally suggest that magnetic resonance imaging might be superior to computed tomography examination for the evaluation of soft tissue abnormalities (Sleutjens et al, 2014; Pease et al, 2017; Veraa et al, 2019).
Scintigraphy
By performing a full clinical evaluation, the segment(s) with pain can easily be identified. Scintigraphic examination is therefore usually not indicated in cervical patients, as it is a screening tool. In patients with vague symptoms where cervical issues may be primary or secondary causes of dysfunction, scintigraphy may show relevant increased radiopharmaceutical capture. Findings should always be correlated to the clinical examination.
Conclusions
A thorough clinical examination can provide detailed information about which structures in the cervical area are affected. A more accurate diagnosis can usually be confirmed with imaging. Radiography and ultrasonography are readily available, but images may lead to under interpretation of existing pathology. Computed tomography is the preferred method of imaging, but one should be careful not to over interpret findings. Cervical pathology is most frequently found in the C5–T1 region and often in more than one location. Findings should always be related to the clinical findings and the presenting complaint to determine their clinical relevance. This requires knowledge of functional anatomy and biomechanics.