

The birth of a foal is a dramatic event. However, as the onlookers are busy assessing the new arrival's potential merits, it is important not to overlook the placenta. This complex, temporary organ has held the responsibility for ensuring that the foal is sufficiently developed and mature to make the transition from an intra-to an extra-uterine existence. During its 11-month gestation, the nutritional requirements of the equine embryo and fetus increase exponentially, and the extra-embryonic membranes (placenta) develop to keep pace with these needs. Initially, the nutritional and excretory exchanges between maternal and fetal tissues takes place via the yolk sac. The yolk sac imbibes the exocrine secretions produced by the endometrial glands. However, the yolk sac soon becomes unable to fulfil the escalating nutritive requirements of the rapidly evolving conceptus and is gradually replaced by the allantochorion. At term, it is this membrane that makes up the bulk of the placental membranes and is the one often referred to as the placenta.
The equine placenta is classified as diffuse (contact of the chorionic microcotyledons occurs over nearly the entire surface of the uterus), epitheliochorial (this refers to the number of layers between maternal and fetal blood and indicates that there is no breakdown of maternal or fetal tissue as occurs, for example, in the placenta of human women) and microcotyledonary (this describes the nature of the chorionic villi that, in the mare, clump and branch to form tiny complex structures that interdigitate with corresponding microcaruncle crypts in the maternal endometrium). The nature of the allantochorion in the mare means that the whole surface of the uterus is required to ensure that there a large enough area of feto–maternal contact to provide enough nutrition to develop and mature a single foal to term. Hence, mares rarely carry twins to term as each twin's placenta has less than the optimum area through which to receive nutrition. For more information on the embryological origins of the yolk sac, allantochorion and twinning, readers are referred to Jeffcott and Whitwell (1973), Whitwell and Jeffcott (1975) and Allen and Wilsher (2009).
This article will focus on examination of the normal term placenta, as it is essential to become familiar with what is ‘normal’, as by appreciating normality, a clinician can recognise abnormality. In addition, the article will discuss some anomalies and their potential implications for the fetus.
The equine placenta – basic morphology
Although the word placenta technically refers to the fetal and maternal components, it refers to just the fetal parts in common usage. Hence, for the purpose of this paper, the fetal membranes will be referred to as the placenta and consist of the allantochorion, allantoamnion (frequently referred to as the amnion), the umbilical cord and a hippomane (Figure 1). The allantochorion corresponds to the shape of the pregnant uterus. During later gestation, the gravid horn contains the majority of the fetus, with the hindlimbs extended to the tip of the gravid horn in late pregnancy. The fetal rump and abdomen would have been located in the area referred to as the greater convexity of the gravid horn (Figure 1). The non-gravid horn does not contain any part of the fetus during late gestation. It is always helpful to keep in mind that the placenta was a three-dimensional structure that contained a fetus and the fetal fluids during gestation.
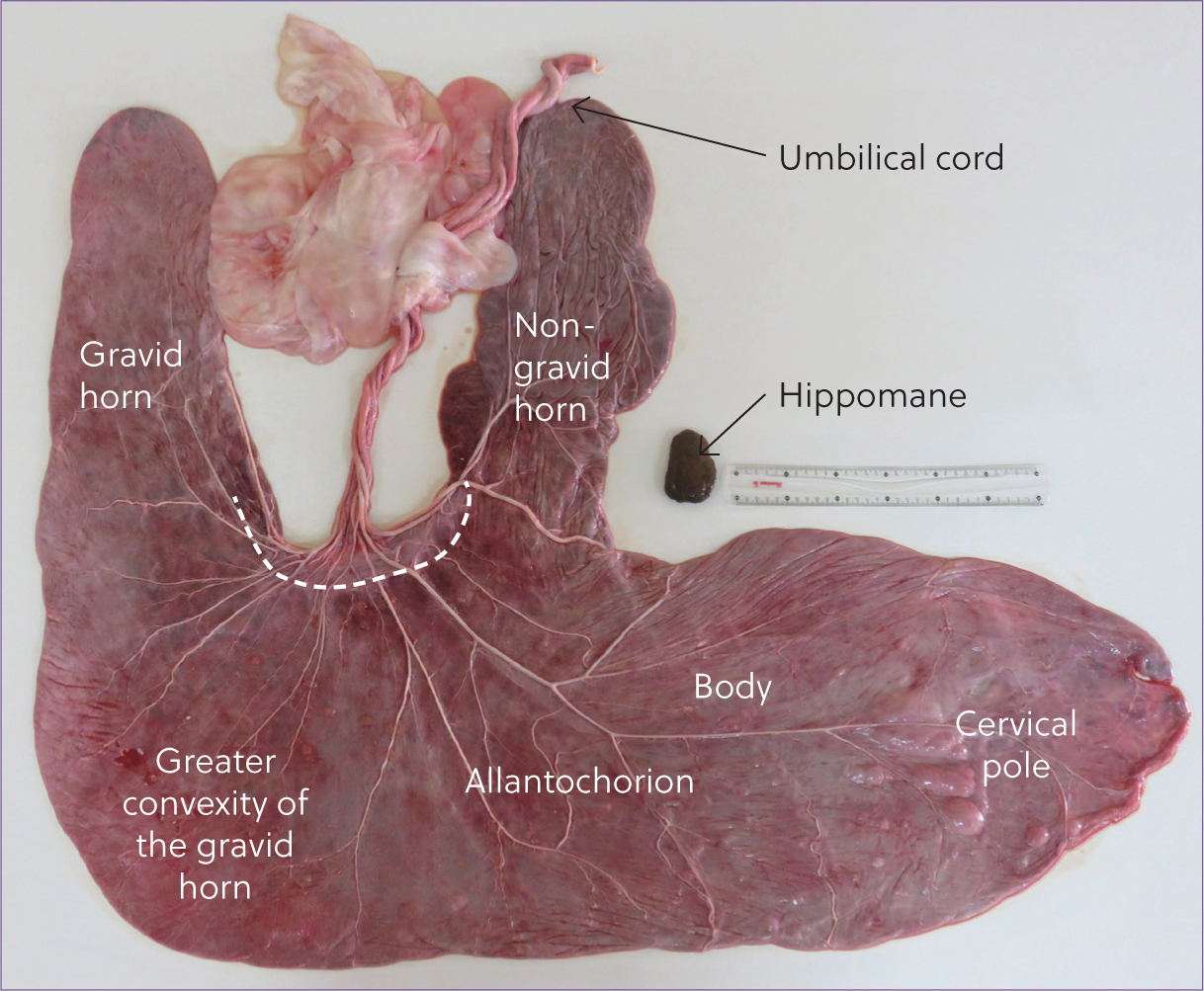
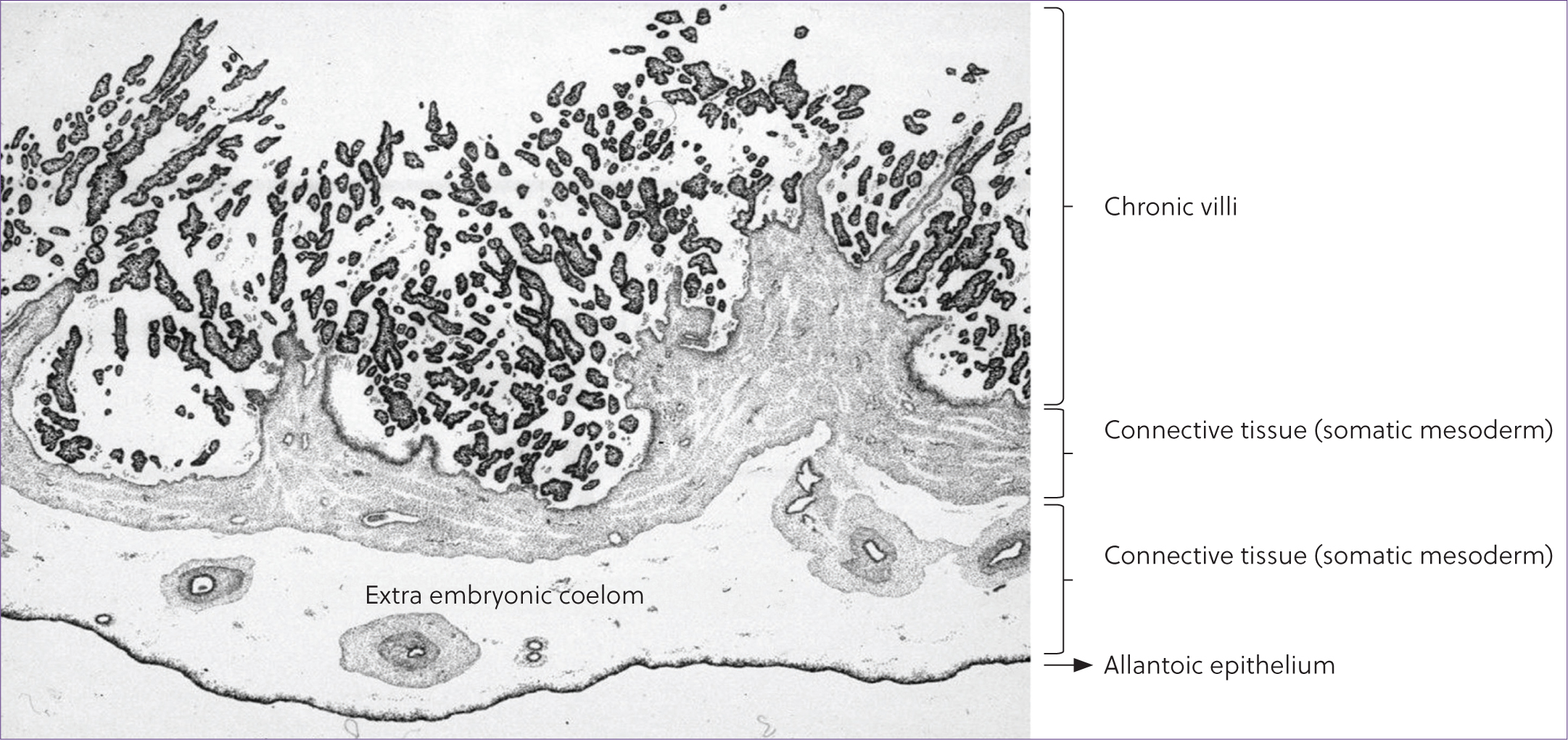
At a microscopic level the allantochorion consists of two layers: the allantois (fetal side; shiny, translucent) and chorion (maternal side; red, velvety side composed of highly vascularised microcotyledons). The layers are partially fused, and the gap between these two layers is known as the extra-embryonic coelom (Whitwell and Jeffcott, 1975; Figure 2). The amnion, or allantoamnion, is also composed of two layers – the amnion and allantois – and surrounds the fetus. Like the allantochorion, fusion between the two layers is not complete. The umbilical cord is usually attached at the bifurcation of the two horns (Figure 1) and, in utero, it provides the conduit from the allantochorion to the fetus so that it can receive nutrition and remove waste products.
The allantochorion and allantoamnion form two cavities during intrauterine life (the allantoic cavity and the amniotic cavity), with the umbilical cord passing through both. The amniotic cavity surrounds the fetus and contains the amniotic fluid which is formed from secretions from the skin, mucus, epithelium fetal saliva and nasopharyngeal secretions of the fetus (Zanella et al, 2014). The allantoic cavity is primarily filled with excretions from the fetal kidneys that pass down the urachus, the thin-walled central portion of the intra-amniotic umbilical cord. In addition, the fetal fluids contain ions, hormones, enzymes and phospholipids produced by the fetus (Williams et al, 1993).
The allantoic cavity also contains a hippomane (Figure 1), which is a soft calculus formed by the concentric deposition of material around a nucleus of tissue debris, composed of desquamated epithelium from the allantoic membrane (Dickerson et al, 1967; King, 1967).
Examination of the placenta
Before examination of the placenta is undertaken, it is important to wear appropriate personal protective equipment to minimise the risk should any zoonotic organisms be present. During the examination, it is best to undertake a systematic approach and helpful to have printed record sheets on which a diagrammatic placental ‘map’ exists, enabling the position of any abnormalities to be recorded accurately. ‘Pictures are worth a thousand words’, so it is useful to photograph anything unusual for later reference. Overall, the examination should focus on completeness and identification of all components of the fetal membranes and any abnormalities that may be present. If abnormalities are detected and sampling of the placenta is undertaken for further investigation, then full thickness pieces of the allantochorion from the cervical star, the body, non-gravid and gravid horns (midway along their lengths) and the base of the gravid horn (the greater convexity) should be fixed in a suitable fixative (eg 10% neutral buffered formalin). In addition, a sample of the umbilical cord (midway between allantochorion and allantoamnion), the allantoamnion and any abnormal areas should be taken. Swabs from the chorionic surface near the cervical star or from any other regions with obvious exudate should also be submitted for bacterial and fungal culture along with sensitivity testing (Schlafer, 2004a; Pozor, 2016a). Although many infections usually result in abortion before term (such as equine herpesvirus-1), it may be prudent to submit samples to rule out such causes even in term deliveries if the placenta appears abnormal or the foal is not healthy.
Reference placental parameters (eg weight of the allantochorion and/or length of the umbilical cord) for different breeds have been documented in several papers (Whitwell and Jeffcott, 1975; Allen et al, 2002; Whitehead et al, 2005; Carluccio et al, 2008; Veronesi et al, 2010; Govaere et al, 2014; Mariella et al, 2018; Robles et al, 2018; Wilsher et al, 2020; Lawson et al, 2024). In general, the weight of the allantochorion is correlated to foal birthweight (Cottrill et al, 1991; Bracher et al, 1996; Allen et al, 2002; Wilsher and Allen, 2003), equating to approximately 6.0–8.3% of the birthweight of the foal (Whitwell and Jeffcott, 1975; Allen et al, 2002; Wilsher and Allen, 2003; Whitehead et al, 2004) and approximately 11% of the entire placental membranes (Schlafer, 2004a). If the examiner only records a limited number of parameters, placental weight (preferably just the allantochorion) and cord length are the ones to detail.
Which side of the placenta was outermost at expulsion?
In most cases the placenta will be passed ‘inside-out’ with the surface outermost (Figure 1) as tension on the umbilical cord during birth inverts the allantochorion. Whitwell and Jeffcott (1975) reported that from 77 Thoroughbred placentae in which the side of expulsion was noted, 58 (75.3%) had the allantoic side outermost. Likewise, Wilsher et al (2020) confirmed this finding in Arabian placentae with 80% (101 out of 127) presenting in this manner. Presentation of the chorionic, villous surface outermost has also been reported to occur more commonly in placentae in which the non-gravid horn is longer than the gravid horn (Whitwell and Jeffcott, 1975), although other studies have not found this correlation (Wilsher et al, 2020). It is believed that placental separation must be initiated at second-stage labour as tension on the cord increases, since the umbilical cord is usually shorter than the uterine body length, yet the foal can lie outside the mare at birth with an unruptured cord (Whitwell and Jeffcott, 1975). The processes that release the allantochorion in its entirety at third-stage labour are poorly understood, but there is certainly variation in the timing of this event among mares. In cases where the allantochorion is released more quickly, it is more likely that they are not so easily everted by tension on the cord. However, presentation of the chorionic surface outermost can be an indication that premature placental separation occurred. This term is used to describe separation of the placenta either before the foal is born or very shortly thereafter. In extreme cases, the allantochorion may fail to rupture at the cervical star (colloquially referred to as a ‘red bag’ delivery). Premature placental separation has a higher incident in induced deliveries (Macpherson et al, 1997; Ousey et al, 2011; Nagel and Aurich, 2022) and in mares experiencing certain conditions (eg placental infections, fescue toxicity and stress; McCue, 2014). The reasons for premature placental separation are unclear, although one study which undertook transcriptomic analysis of allantochorions from mares with premature placental separation reported changes in the expression of genes between premature placental separation and control placentae (Murase et al, 2023). The overall consideration is that, although in many cases presentation of the placenta with the chorionic red surface outermost may not be of any consequence for the foal, it should alert the examiner to the possibility that the allantochorion may have detached prematurely. Premature detachment of the allantochorion may predispose the foal to problems associated with hypoxia, even though the foal may appear normal at birth (McCue, 2014).
Is the allantochorion complete?
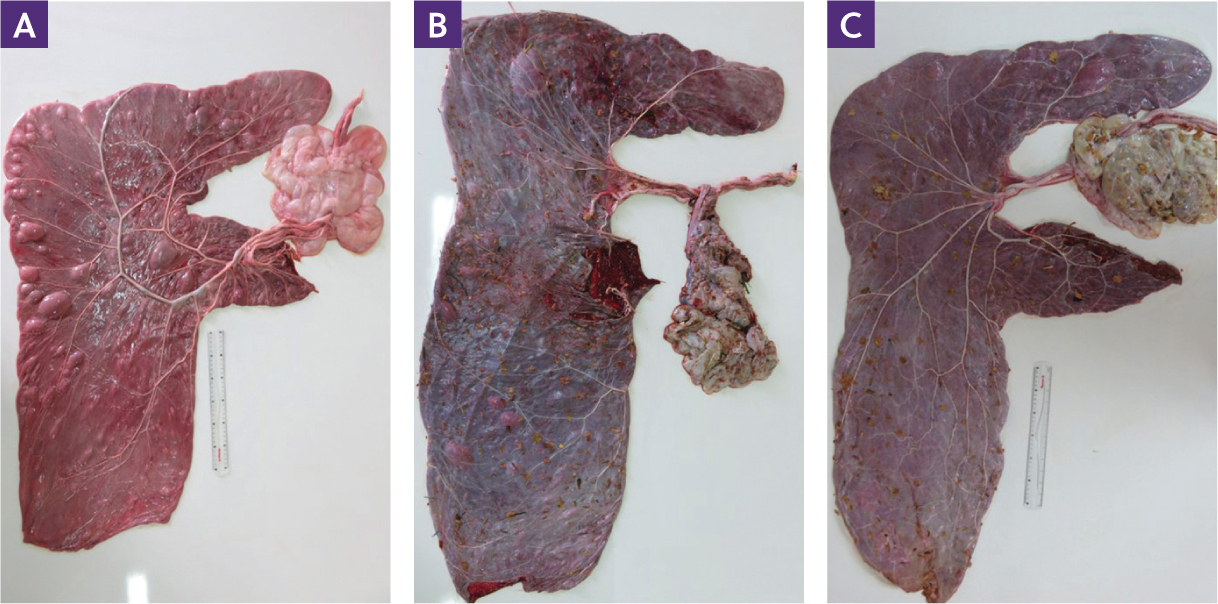
One of the most important reasons for checking the placenta is to assess if it is complete. Retention of the fetal membranes is the most common postpartum complication in mares (Frazer, 2003; Lopate, 2003). Usually, the diagnosis is relatively easy to make when the entire allantochorion fails to detach and be passed within 3 hours of parturition (LeBlanc, 2008). However, the allantochorion may tear and a portion be left in situ, with the tip of the non-gravid horn being the region which is usually retained (Figure 3; Vandeplassche et al, 1971; LeBlanc, 2008), with the suggestion that the greater depth of the microcotyledonary villi in the non-gravid horn and increased folding may be partly responsible (Vandeplassche et al, 1971; O'Brien, 2015). Others have proposed that the thinner nature of the non-gravid horn compared to the gravid one, and the fact it is normally expelled last, make it more likely to be torn and retained (Pozor, 2016a).
In the authors opinion, it is easiest to lay the placenta out in an F-configuration (Figure 1) to check for completeness and to allow further examination. Initially, the allantoic (fetal) surface is outermost so that the umbilical cord and amnion are fully exposed. Subsequently, the allantochorion is inverted to examine the chorionic (maternal or villous) surface. A natural inclination will exist as to whether the allantochorion lies with the arms of the F to the right or left depending on which uterine horn was the gravid one. To determine this, with the allantoic surface outermost, grasp the tips of the two horns with the cervical pole closest to the operator and lift the horn tips up so the rest of the allantochorion hangs downwards. The base of the gravid horn should then hang down, rather like the heel of a sock held at the toe end. Since the allantochorion is in effect inside out if the allantoic surface is outermost, if it is the right side that hangs down then the left uterine horn would have been the gravid one, and vice versa. As the allantochorion, in effect, mirrors the health of the underlying maternal endometrium, orientating the horns provides invaluable information as to where any intrauterine problems may lie should anomalies be found on the allantochorion.
Once the placenta has been placed in the F-configuration there should only be one opening in the allantochorion at the cervical pole, and examination of the chorionic side in this region will reveal the avillous lines corresponding to where the chorionic surface abutted against the internal os. Figure 3 shows examples of placenta in which portions of the non-gravid horn has been retained. If a proportion of the allantochorion has been retained, appropriate measures should be taken (Canisso et al, 2013; Burden et al, 2019) because the retention of a portion of the allantochorion is as dangerous for the mare's wellbeing as the whole placenta being retained – perhaps more so, as it can easily go unnoticed until clinical signs become apparent. Any piece of retained allantochorion will quickly begin to autolyse and form a nidus of bacterial growth from which toxins are produced and absorbed by the mare. Untreated or undiagnosed retention of all or part of the allantochorion can therefore lead to endotoxaemia with resulting laminitis, metritis, septacaemia or death (Canisso et al, 2013; Pozor, 2016a).
Is the allantochorion complete but torn?
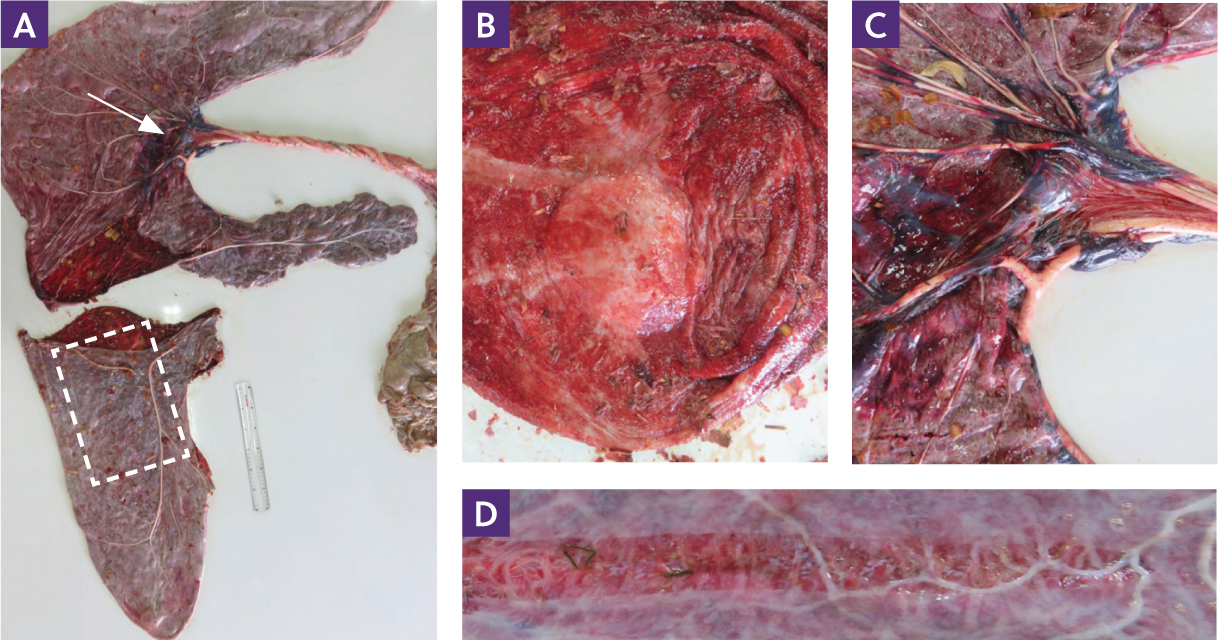
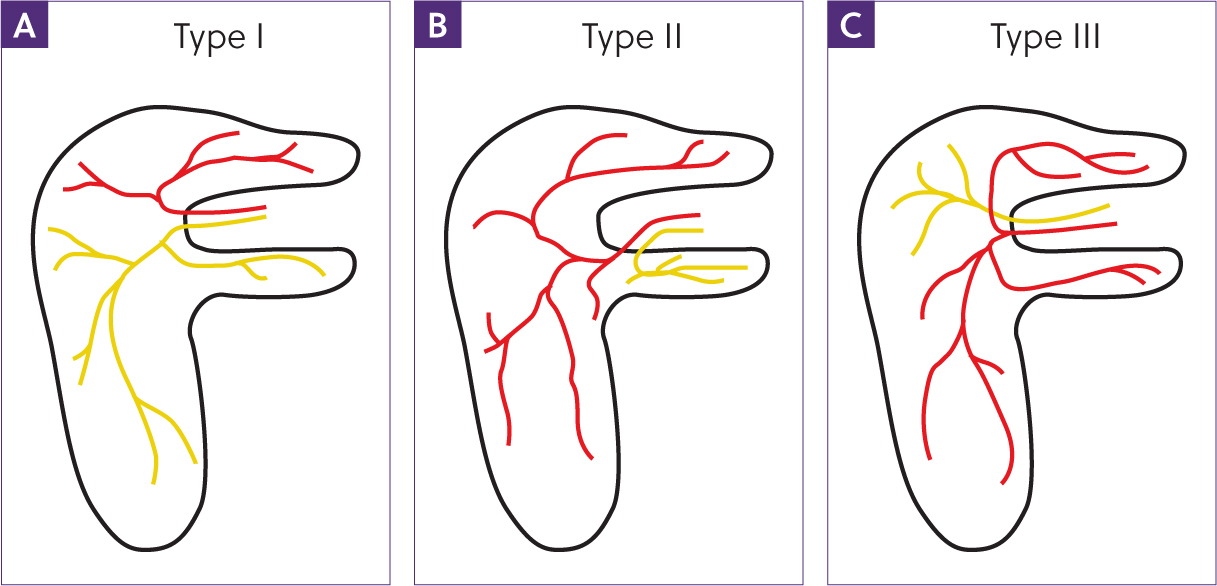
Sometimes, the allantochorion is complete but torn. Some tearing can occur when the mare inadvertently stands on the membranes and, with care, it is usually possible to match major vessels either side of the tear (when the allantochorion is viewed from the allantoic side) to assess if there is any missing piece. If the clinician is in any doubt as to whether all the allantochorion has been passed, the mare should be examined and lavage undertaken to ensure that any retained pieces have been recovered. Major tears may also occur when the cervical pole is grossly thickened and fails to rupture (Figure 4a); for example, in cases of placentitis or placental oedema (Williams, 2012). As parturition occurs, the failure of the cervical star to rupture (premature placental separation, often also referred to as a ‘red bag’) combined with the increasing forward push from uterine contractions results in the allantochorion rupturing at the next weakest point. This is usually through the anterior portion of the body at the base of the horns. This pattern of tearing is often accompanied not only by an intact cervical star region, but also stress lines, with rupture of the allantoic surface in the body region and frequently blood within the extra-embryonic coelom (Figure 4b–d). Such a placenta should alert the examiner to the likelihood that the foal may have suffered periparturient fetal hypoxia and be compromised. Although these foals may appear normal at birth, they are at risk of developing hypoxic ischaemic encephalopathy (also sometimes referred to as neonatal maladjustment syndrome or dummy foal syndrome). Such foals may have trouble standing, show a poor suck reflex, fail to find the teat to suck, have an abnormal swallowing reflex, head tilt, walk in circles, show reduced gut motility which can result in meconium impaction or reflux of ingested milk, abnormal bladder function and/or kidney failure. In addition, they are more susceptible to infections (Toribio, 2019).
The shape and overall appearance of the allantochorion
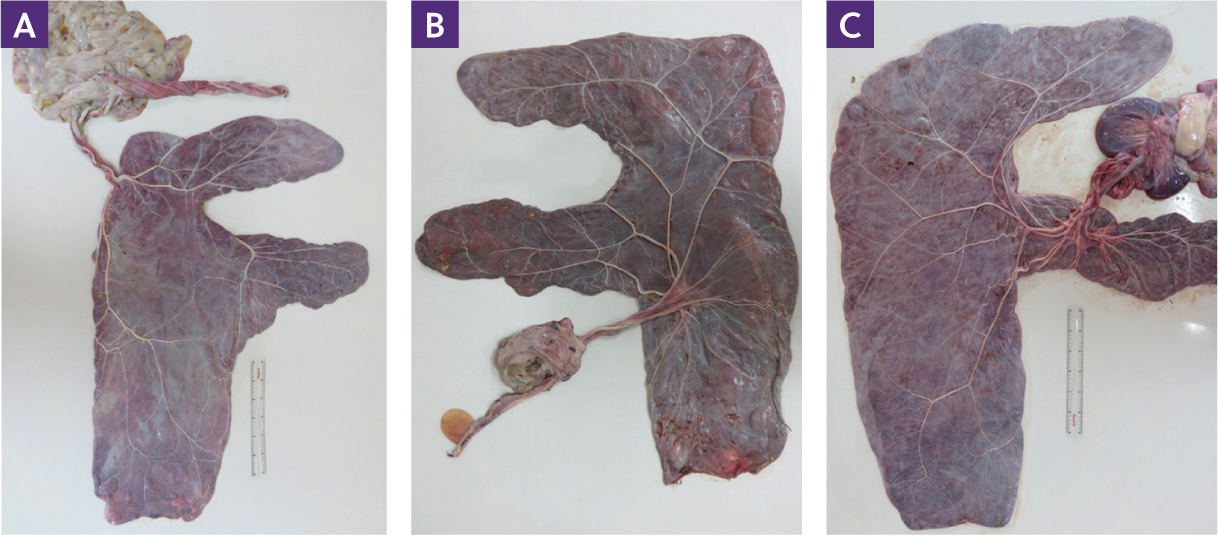
When the placenta has been laid out in the F-configuration, it gives some indication as to the shape of the uterus during late gestation. Although in most instances twins are aborted before term, it is possible for one twin to die in utero or be reduced after 40 days (Wolfsdorf and Macpherson, 2010) while its co-twin survives to term. In such a scenario, the allantochorion will show tell-tale signs. These may include an abnormal shape to the allantochorion, avillous areas as a result of twin juxtaposition or an invagination with a mummified twin (Jeffcott and Whitwell, 1973; Ball et al, 1993; Rapacz-Leonard and Paździor-Czapula, 2022).
Linear dimensions of the allantochorion in an F-configuration have been reported for both thoroughbreds (Whitwell and Jeffcott, 1975) and Arabian mares (Wilsher et al, 2020). However, these measurements are subject to inconsistency as to how the placenta is laid out and their true clinical relevance is not known. Despite this, the overall shape of the allantochorion can provide clues as to the positioning of the fetus in utero and/or uterine ‘moulding’ of fetal position, giving possible reasons for malpresentations leading to dystocia or congenital deformities (Rooney, 1966; Fackelman, 1984; Whitwell, 1987; Wilsher et al, 2013; Newcombe and Kelly, 2014; Valli et al, 2022). For example, in one study examining the placentae of eight Thoroughbred foals born with congenital flexural limb deformities, the allantochorions showed reductions in their linear dimensions and folding over the course of major blood vessels indicative of uterine restriction (Wilsher et al, 2013). However, although similar findings have been reported by other authors (Rooney, 1966; Fackelman, 1984; Whitwell, 1987), it is difficult to distinguish between cause and effect. Hence, are the changes observed in the allantochorion a reflection of uterine restriction causing fetal deformities, or such deformities altering the shape of the placenta as fetal movements become restricted? Nevertheless, abnormalities of the shape of the allantochorion should be noted, especially when fetal deformities or malpresentation are present (Figure 5).
The thickness of the normal allantochorion will vary across its surface, with the non-gravid horn appearing thinner than the gravid horn and body regions. Furthermore, the non-gravid horn frequently has a ‘puckered’ appearance because it has not been as stretched to the same degree as the gravid horn during pregnancy. Oedema and thickening are a common feature at the tip of the gravid horn, and lesions known as placental area of degeneration because of chronic repetitive trauma from the fetal hind feet are a frequent finding (Schlafer, 2011). However, if such lesions or thickening are present in excess or in other areas (especially near the cervical star) they should be viewed suspiciously.
The allantoic surface of the allantochorion
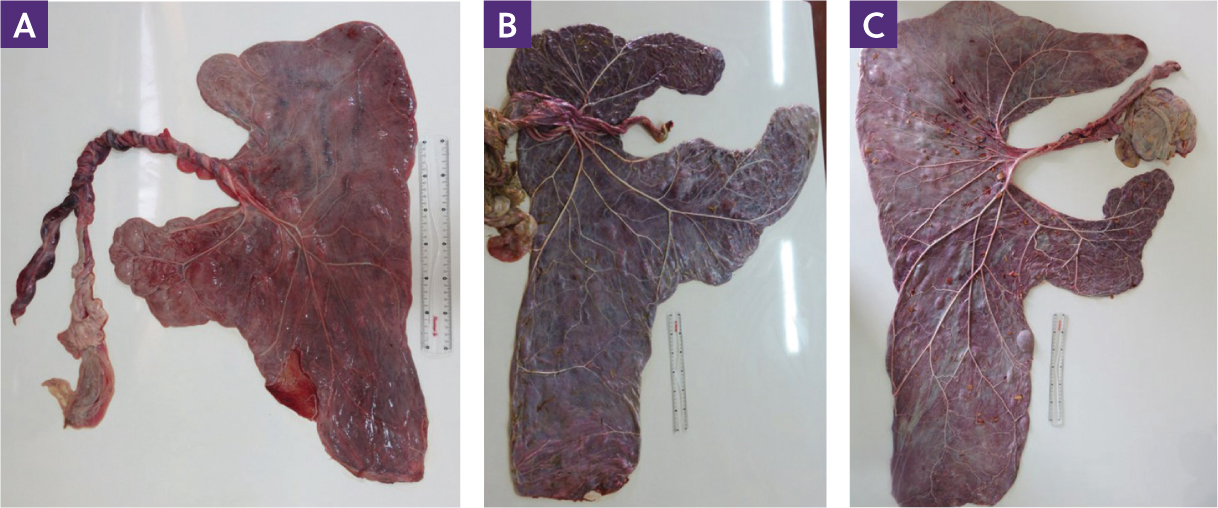
The vascular network of the placenta can be appreciated from the allantoic surface, and a multitude of vessels can be seen across the allantochorion between the chorionic and allantoic surfaces. The major vessels that radiate out from the site of attachment of the umbilical cord generally follow three different patterns, as described by Whitwell (personal communication in Rossdale and Ricketts, 2002) (Figure 6). These delineate the relative area of the allantochorion that each of the two umbilical arteries and veins vascularise. However, variations exist; one perfusion study injecting different coloured dyes into the two umbilical arteries demonstrated that some areas of the allantochorion are vascularised by both sets of umbilical arteries and veins (Cottrill et al, 1991). The significance of the type of vascular pattern on the function of the allantochorion is not known. Whitwell originally suggested that the type III pattern may be associated with twin reduction during early pregnancy (personal communication in Rossdale and Ricketts, 2002), although other authors have not found such a link (Whitehead et al, 2004).
Other features that may be present on the allantoic surface are out-pouchings, which may be fluid-filled. These generally take three forms: folding of the allantochorion over a major vessel, an excess of fluid remaining in the extra-embryonic coelom (allantoic pouches or vesicles) or folding of the allantochorion over the remnants of the endometrial cups (allantochorionic pouch or endometrial cup pouch; Clegg et al, 1954; Whitwell and Jeffcott, 1975; Pozor, 2016b). Allantoic pouches are frequently located along the course of major vessels and may range in size from a few centimetres to so-called mega structures up to 15 cm in diameter (Singh et al, 2009). It is assumed that allantoic vesicles are clinically inconsequential, but there is a lack of information on how the placental membranes maintain a degree of fluid homeostasis, especially bearing in mind there is no placental lymphatic system. However, water channels (aquaporins) are present on the equine allantoamnion and allantochorion (Wilsher and Allen, unpublished findings), and these may play a role in maintaining fluid balance within and between the different placental compartments.
Tags of hippomane may also be adhered to the allantoic surface (Whitwell and Jeffcott, 1975). A roughened, discoloured area may also be apparent to the tip of the gravid horn, sometimes with dystrophic calcification. This has been suggested to occur because of pressure from the fetal hooves (placental area of degeneration lesions; Schlafer, 2011), or may be a consequence of adaption of the allantochorion in the area which is subjected to considerable tension from the weight of the fetus.
The chorionic surface of the allantochorion
The chorionic (maternal/villous) surface is perhaps more revealing in terms of fetal wellbeing than the allantoic surface, as it is covered in a myriad of microcotyledons, the exchange units of the placenta. The microcotyledons are highly vascularised, multibranched villi, which interdigitate with corresponding crypts in the maternal endometrium, and give the chorionic surface its red, velvety appearance. Microcotyledons are present over the majority of the chorionic surface, with the exception of areas which develop against uterine epithelium devoid of endometrial glands. Namely, those areas that overlie the utero–tubal papillae at the tips of the uterine horns, the area overlying the internal os of the cervix and the areas overlying the endometrial cups. In addition, since microcotyledons only develop against functional endometrium, sub-optimal endometrial health in the form of scarring or age-related endometriosis leads to the formation of poorly developed microcotyledons or no development at all (Bracher et al, 1996; Wilsher and Allen, 2003; Wilsher et al, 2019). Furthermore, since the growth factors produced by the lumenal and glandular uterine epithelium that initiate villous formation are stage-related during gestation, late expansion of the allantochorion to occupy the uterine lumen as a result of late twin reduction (either natural or elective) also results in poor microcotyledon development (Ball et al, 1993; Govaere et al, 2008; Rapacz-Leonard and Paździor-Czapula, 2022).
The height and density of the microcotyledons also varies across the allantochorion, with the villi closely packed together in the non-gravid horn, or widely spaced, as occurs on the convexity of the gravid horn corresponding to the area where the rump of fetus has been resting. The colouration of the chorionic surface can also vary greatly, ranging from a bright red to a muddy brown (Figures 7a; 7b). These variations, often in clearly demarcated areas, are not uncommon and relate to the height and density of the villi and the degree of blood stasis in their microvasculature (Figure 7b; Whitwell and Jeffcott, 1975), and the time from expulsion to examination of the allantochorion. Villous areas that have lost their intimate contact with the endometrium, such as at the tip of the gravid horn, may be covered with a sticky exudate or show calcification. However, the presence of exudate covering large areas is abnormal. A severe, focal, mucopurulent exudate and necrotising tissue above a well-defined avillous area on the ventral aspect of the base of the gravid horn/uterine body is indicative of nocardioform placentitis – a significant cause of focal placentitis in parts of the USA but rarely documented elsewhere (Foote et al, 2012). Focal placentitis may also be related to haematogenous spread from the mare (Foote et al, 2012). Exudate or changes in the villous surface extending forward from the cervical pole region should also alert the clinician to the possibility of an infective placentitis (Figure 7c) or necrosis of the cervical pole region, occasioned by excessive cord length (Foote et al, 2012). Bacteria commonly associated with placentitis include Streptococcus equi ssp. zooepidemicus and Escherichia coli (Hong et al, 1993; Smith et al, 2003). However, any opportunistic bacteria that gain entry through the cervical canal can cause placentitis. As a residual bacterial infection is common after placentitis, cytology and culture of endometrial swab is also advisable. Fungal placentitis also occurs, but less frequently than bacterial, with Aspergillus and other mucor species being the most common offending organisms (Hong et al, 1993).
The allantoamnion – or amnion
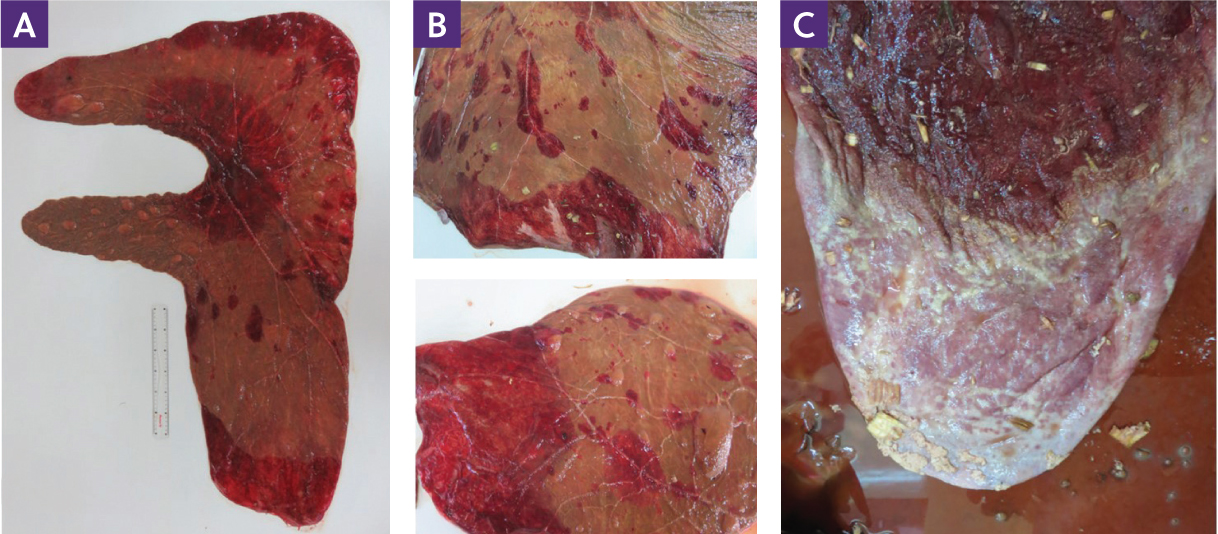
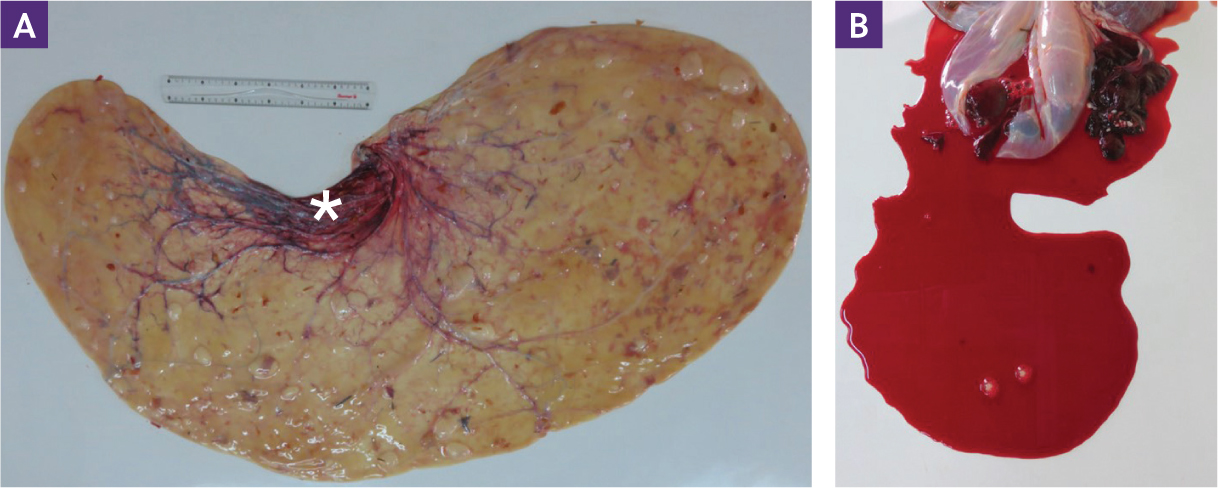
The amnion is a white, glistening membrane with numerous and tortuous prominent vessels emanating from where the umbilical cord passes through it. At term, its surface area is greater than that of the allantochorion and, when laid out, it has a distinctive comma shape with the umbilical cord at the centre of the concavity (Whitwell and Jeffcott, 1975; Figure 8).
The amnion should be assessed for uniform thickness and colour. A yellow or brown tinge usually indicates staining by meconium which may be an indicator of fetal stress at or near the time of parturition (Schlafer, 2004a; Figure 9). Although localised oedema is often seen, widespread oedema and thickening can be associated with fetal compromise. A large amount of free and clotted blood within the amnion may indicate the cord ruptured prematurely and the foal failed to acquire all the blood from the placenta at birth (Figure 9b).
Amniotic plaques, also referred to as pustules or hyperplastic nodules, are a common finding on the inner surface of the amnion and on the outer surface of the amniotic segment of the umbilical cord (Figure 8c). Calcified plaques may be observed as a consequence of a reaction to adhered hippomane material. Amnion nodosum, a condition in which granular amorphous nodules are found on the surface of the thickened amnion, has also been described in the mare with no apparent adverse effects for the foal (Govaere et al, 2011).
Umbilical cord
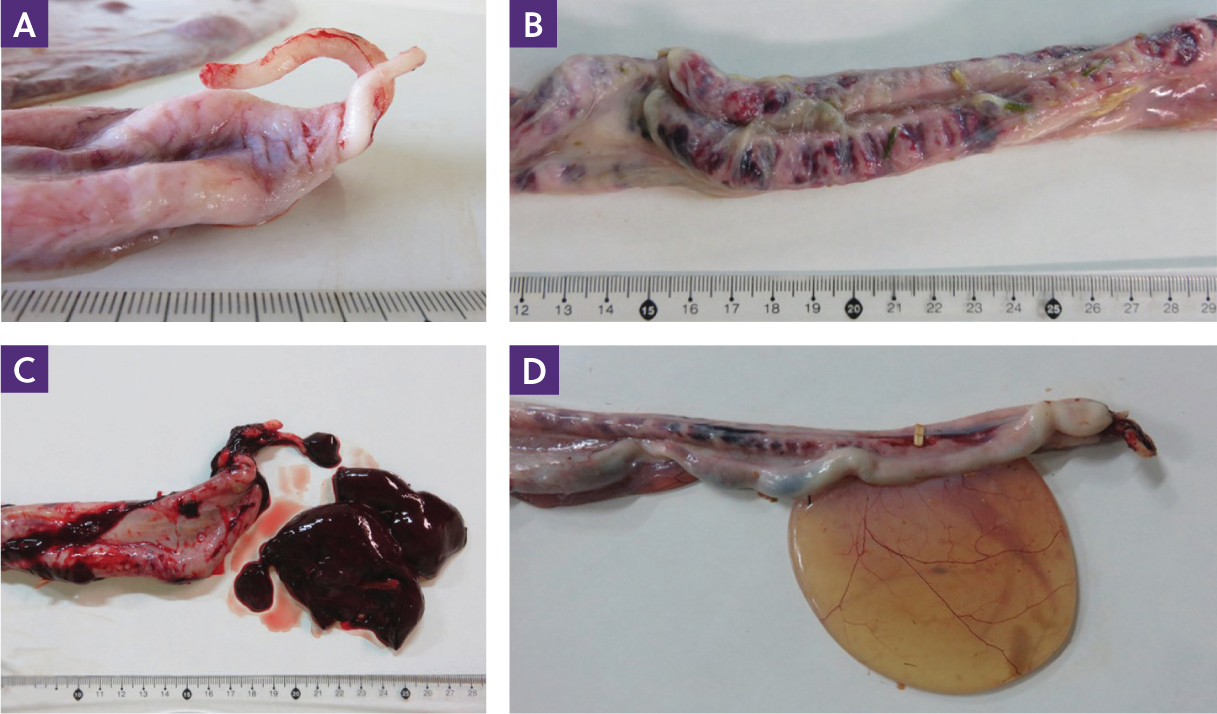
The umbilical cord is the conduit through which the fetal blood carries the nutrients and oxygenated blood to, and all the gaseous and metabolic waste from, the developing fetus. Hence, any shortfalls or variation in its morphology will have a direct influence on fetal development and health. A natural break of the cord is indicated by two worm-like arterial walls projecting from the fetal end of the cord (Figure 10a; Whitwell and Jeffcott, 1975). The absence of these structures, particularly when large blood clots are present on the end of the cord, should alert the examiner to the possibility that the cord ruptured prematurely (Figure 10b). In addition, the navel stump of the foal should be checked carefully to ensure that it has sealed correctly and is not patent.
The umbilical cord is usually located dorsally at the bifurcation of the uterine horns (Figure 1) or just within the entrance to the gravid or non-gravid horn and reflects the position where the conceptus became fixed, around day 16–17 after ovulation. The dorsal positioning ensures that the enlarging fetus will not lie upon the cord and potentially occlude its blood flow in later gestation. Abnormal cord attachment can occur when the embryonic vesicle becomes fixed in an unusual place (Wilsher et al, 2020), eg in the uterine body (Joubert et al, 2005), at the tip of a uterine horn (Wilsher et al, 2009) or as a consequence of dorsal positioning of the embryo during early development, resulting in ventral attachment of the cord (Figure 11; Ginther, 1983; Wilsher et al, 2009).
The umbilical cord comprises a proximal intra-amniotic portion attached to the fetus and a distal allantoic portion attached to the allantochorion. The amniotic portion contains two umbilical arteries, an umbilical vein and the urachus. The allantoic portion contains two arteries and two veins; the veins unite at the proximal end of the allantoic portion or just inside the amniotic cavity. A disparity in the size of the umbilical arteries has been noted by several authors to occur as a result of variability in the area of the allantochorion each vessel is associated with (Whitwell, 1975; Whitwell and Jeffcott, 1975; Wilsher et al, 2009). Anomalies in the number of major blood vessels in the umbilical cord are well documented in humans and have been associated with both placental abnormalities and congenital problems in the human neonate. In the mare, the absence (Whitwell, 1975; Girodroux et al, 2019) and aplasia (Wilsher et al, 2011) of one umbilical artery has been reported. In addition, supernumerary of the major umbilical vessels has also been described (Wilsher et al, 2011).
In Thoroughbred foals, the mean length of the umbilical cord has been reported as 55 cm, with a range of 32–90 cm (n=143; Whitwell and Jeffcott, 1975). Similar values have been ascribed to Standardbred mares (59 cm, range 32–152 cm, n=84; Whitehead et al, 2004). Interestingly, despite their smaller stature compared to Thoroughbreds, Arabian mares have been reported in one study to have a significantly longer umbilical cord than thoroughbred mares (62.2 cm, range 38–105 cm, n=127; Wilsher et al, 2020). However, umbilical cord length in pony mares is considerably shorter than in Thoroughbred mares (41 cm, range 30–48 cm, n=10; Whitwell and Jeffcott, 1975).
Particularly short cords (ie <40 cm) may predispose the foal to premature cord rupture during delivery and resulting intra-partum anoxia. Cord length tends to be longer if the attachment is in the non-gravid horn. Excessive cord length can result in many problems, including strangulation of the cord around the fetus, excessive torsion (indicated by alternating bands of congestion and blanching along the cord length) and allantochorionic necrosis at the cervical pole (Whitwell, 1975; Frazer, 2007; Foote et al, 2012). Although there is little information as to the factors which influence cord length in the horse, genetics and gestation length are known to play determining roles in humans. Furthermore, short cords are more common in people in situations of decreased fetal movement as a result of congenital anomalies, intrauterine restriction or administration of certain drugs (Katz et al, 1987; Baergen, 2005). Longer cords are more common where amniotic fluid volume is increased and fetal movement potentially increased (Ogita et al, 1989).
Twisting, sometimes referred to as natural spiralling or chirality, of the vessels is a common finding in the equine umbilical cord. It originates from fetal movements before 7–8 months of gestation after which the fetus becomes too large to rotate within the uterus (Ginther and Griffin, 1993; Bucca et al, 2005). One study of 157 equine placentae reported that 78% of the cords were twisted, with a mean of 4.4 twists per cord (Vandeplassche and Lauwers, 1986). Twisting in the amniotic and allantoic portions of the cord occurs independently and can be in opposite directions. Hence, twisting may be observed in just one portion of the cord. Excessive twisting of the cord can lead to obstruction of the blood vessels and fetal death, but even mild twisting will alter the fluid dynamics of the blood passing along its length. Furthermore, twisting of the cord in the amniotic portion can lead to dilation or obstruction of the urachus (Figure 10d), with or without bladder distension. In humans, umbilical cord twisting occurs much more commonly in a counter-clockwise direction (ie a ‘left’ twist; Baergen, 2005), but in the mare there appears to be no preferential direction (Vandeplassche and Lauwers, 1986).
Yolk sac remnants
A yolk sac remnant can be found on every placenta, but it is rarely observed because, in most instances, it is a thread-like structure hidden within the infundibulum (Figure 12a). Careful dissection into the infundibulum, the funnel shaped cavity where the umbilical cord joins the allantochorion, will reveal its presence (Figures 12a; 12b). On occasion, the remnant grows in size, and may reach a diameter up to 20 cm and weigh over 1 kg (Figure 12c; Wilsher et al, 2020). Such structures are invariably ossified and/or may be filled with a bloody, serous fluid (reviewed in Vilaregut et al, 2021). Furthermore, should the attachments that secure an enlarged yolk sac within the infundibulum break or stretch, they can migrate to a variety of positions in the fetal membranes (Vilaregut et al, 2021).
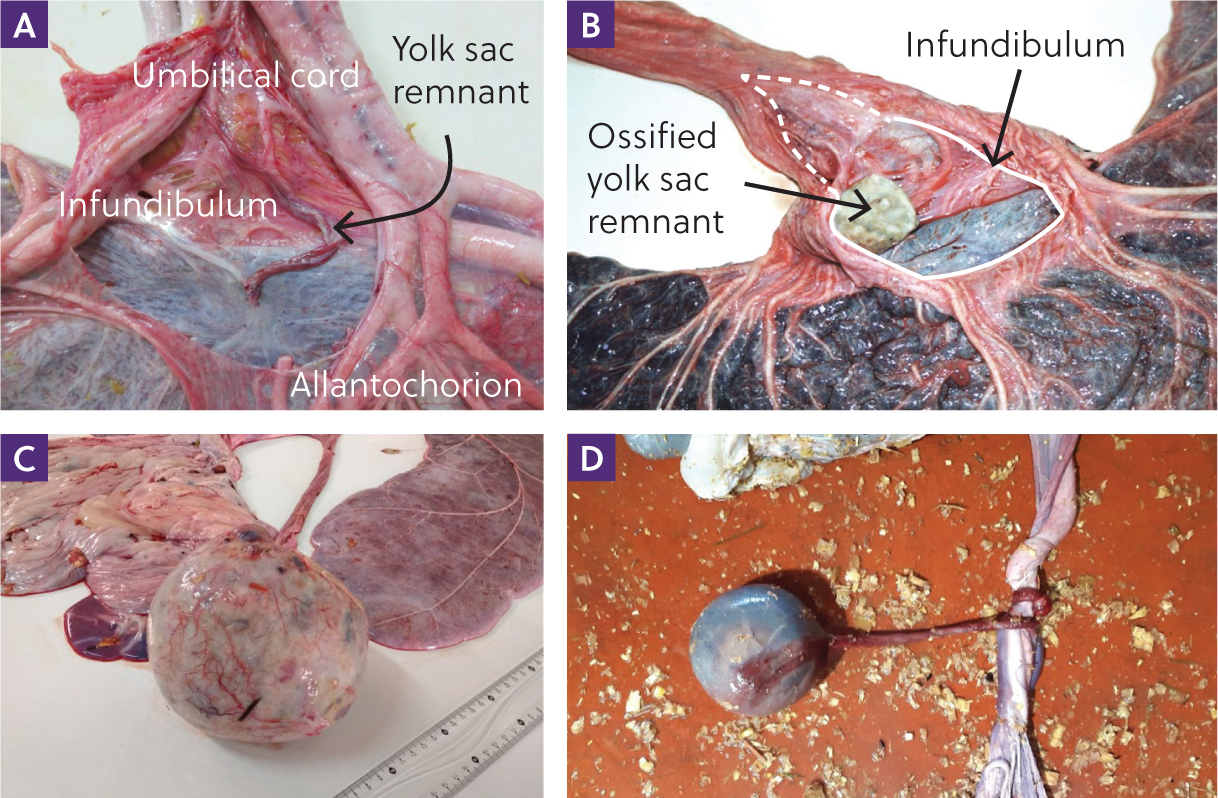
The inexperienced examiner may mistake a yolk sac remnant for a blighted twin or the equine equivalent of the bovine amorphous globulus (Crossman and Dickens, 1974). However, they are not such structures, and are believed to form as a consequence of metaplastic changes that start in the involuted remnants of the yolk sac (Schlafer, 2004b). Although yolk sac remnants are not usually considered to cause any untoward problems for the mare or foal they have been implicated in abortion as a result of physically compromising the blood flow through the umbilical cord (Figure 12d; Schlafer, 2004b; Vilaregut et al, 2021).
Hippomanes
The hippomane (also referred to as an allantoic calculi, planter's cushion, foal's bread or foal's tongue) is a soft, rubbery, flat, oval structure (Figure 13a) which is formed from a core of desquamated epithelium from the fetal membranes onto which is deposited concentric layers of debris from the allantoic fluid. It contains high concentrations of nitrogen, calcium, phosphorous, sodium, potassium and magnesium (Dickerson et al, 1967). Usually, only a solitary hippomane is present, that is first found in the allantoic fluid around day 85 of gestation and which increases in size from little more than a centimetre in length to as much as 14 cm at term (King, 1967).
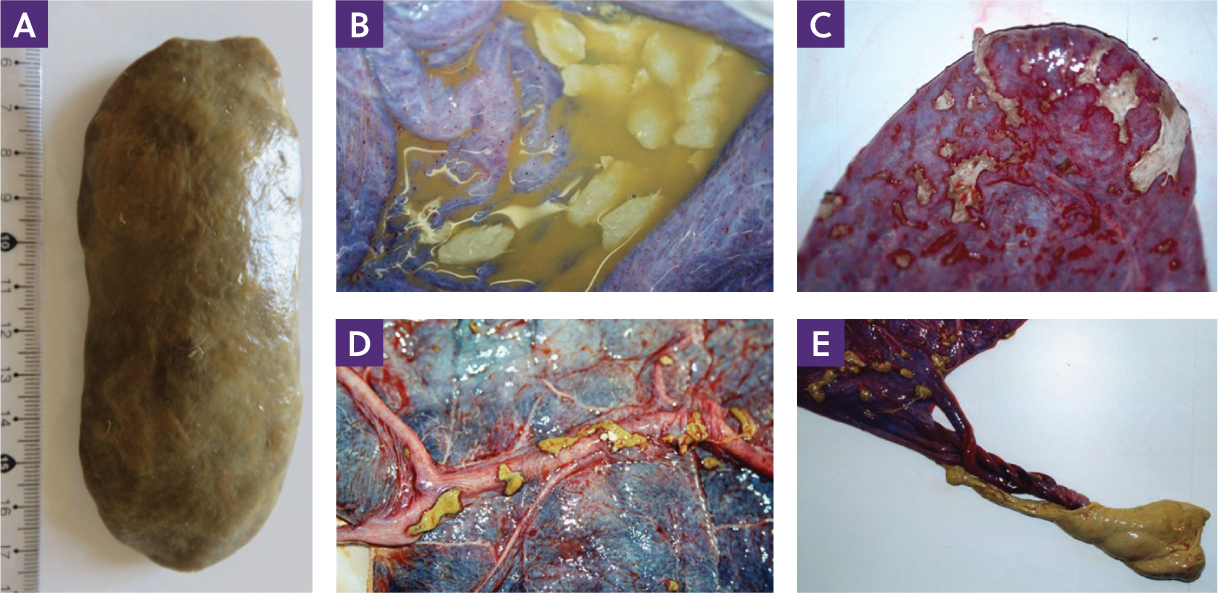
Hippomanes have a higher specific gravity than allantoic fluid, so they lie on the floor of the allantoic cavity. Here, allantoic debris tend to gravitate and adhere to the single hippomane which becomes moulded and flattened as pregnancy advances by the increasingly confined space between the allantoamnion and allantochorion. At term, the hippomane varies in colour from off-white through khaki to dark brown. Small deposits of hippomane material can adhere to other parts of the placenta (Figures 13b–e) and are commonly seen on the allantoic surface at the tip of the gravid horn and near the cervical pole. Whitwell and Jeffcott (1975) noted that approximately 8% of allantoamnions had circular calcified areas corresponding to where hippomane material had adhered to the allantoic surface. These are not usually considered a problem, although the author has seen placentae in which the allantoamnion has ruptured as a consequence of such reactions. These cases tend to have numerous sticky hippomanes, rather than a single discrete one.
Conclusions
Routine examination of the fetal membranes at term should be encouraged, even when nothing appears amiss with the foal. Clinicians should not only check for completeness but also undertake a methodical examination so that the normal morphology of this organ is well understood. Hence, when abnormalities occur, they will be noted much more readily.