

Halicephalobus gingivalis belongs to the nematode order Rhabditida, family Paragrolaimidae. Currently, there are eight described species of Halicephalobus, but only H. gingivalis is known to infect mammals (Onyiche et al, 2017). This nematode is a ubiquitous, saprophytic, free-living, rhabditiform parasite of soil and manure that has been associated with opportunistic infections in horses, but sporadically also in zebras, cattle and humans (Enemark et al, 2016; Onyiche et al, 2017). The species was named by Stefanski (1954), who found the worms in a granuloma in the gingivae of a horse in Poland. Only parasitic female adults, larvae and eggs have been observed in parasitised hosts, indicating that H. gingivalis may reproduce parthenogenetically, although how H. gingivalis infects equine and human hosts is still largely unknown (Papadi et al, 2013). Human infections are very rare, but all cases described to date involved meningoencephalitis with an invariably fatal outcome (Lim et al, 2015). H. gingivalis infection in horses has been reported worldwide, usually involving a wide range of ages (from colts to aging adults) and breeds (Anderson et al, 1998; Monoranu et al, 2015). Among the reported equine cases, only four horses have survived (Dunn et al, 1993; Pearce et al, 2001; Schmitz and Chaffin, 2004; Muller et al, 2008). In Europe, the disease has been reported in several countries, including the UK, Belgium, Italy, Denmark, Spain, Iceland, Romania, Portugal and Sweden. Table 1 summarises reported H. gingivalis cases in equids to date.
Phylogeny
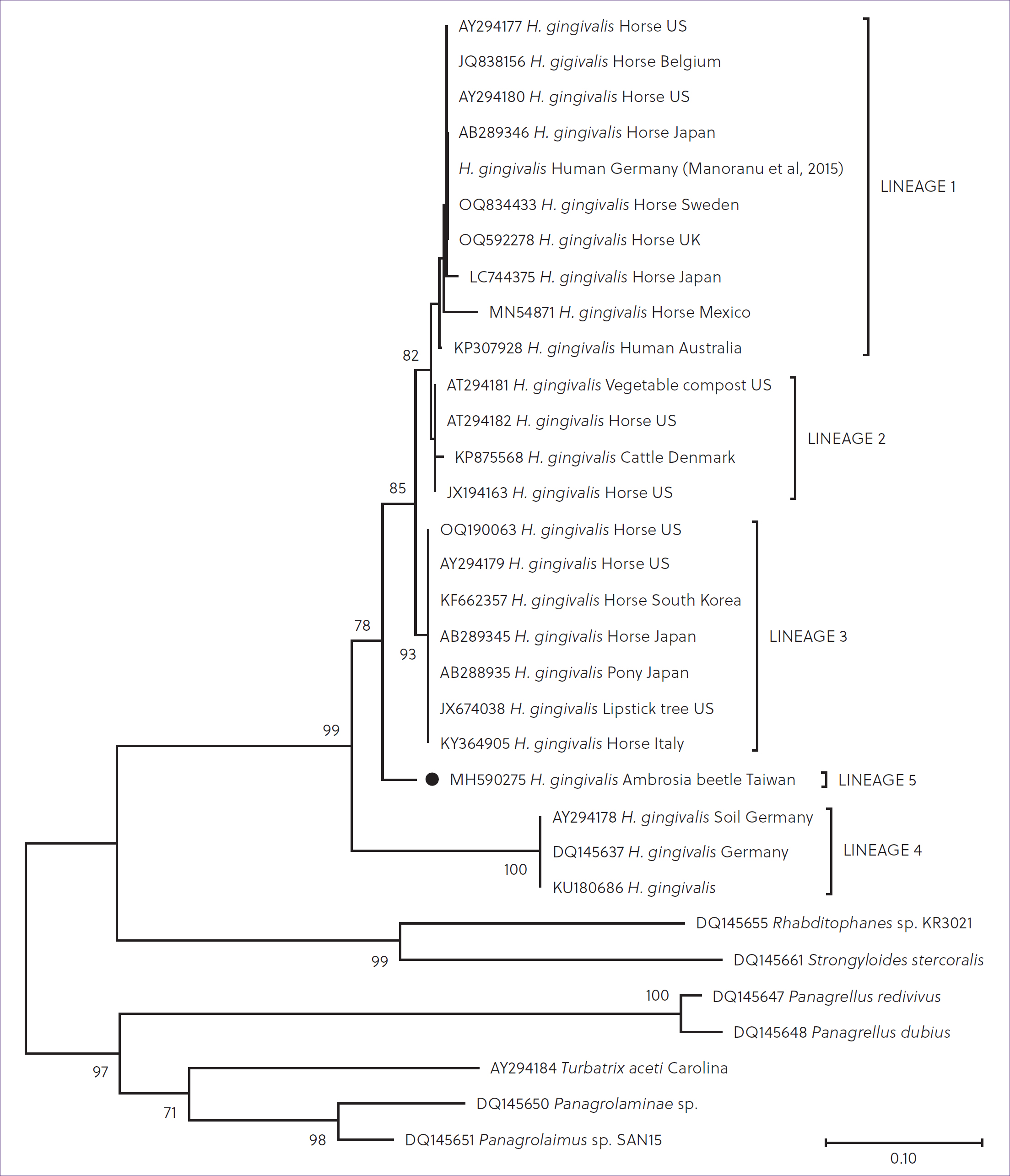
Phylogenetic analysis of rDNA sequences revealed that isolates representing the morphospecies H. gingivalis consist of at least four genetically distinct evolutionary lineage (Nadler et al, 2003).
However, this observation relies on a limited number of sequences available on public databases, with little information on date of sample collection and location. Only a few case studies performed molecular typing of the parasites (Akagami et al, 2007; Jung et al, 2014; Taulescu et al, 2016; Pintore et al, 2017; Avila et al, 2020; Baker et al, 2023; Olofsson et al, 2023). Current knowledge on H. gingivalis phylogeny shows that Lineage 1 includes isolates from Europe, North America, Japan and Australia. The isolate identified in cattle in Denmark belongs to Lineage 2, as well as an equine isolate from the US. H. gingivalis isolates belonging to Lineage 3 were detected in Italy, Japan and the US. Finally, German isolates cluster within Lineage 4 (Figure 1) (Nadler et al, 2003; Pintore et al, 2017; Olofsson et, 2023). However, sequence similarity data and phylogenetic analysis confirm that there is no correlation between location and genetics in H. gingivalis based on 28S rRNA gene data. This result shows that single geographic regions may contain a diverse pool of isolates capable of infecting horses, and that halicephalobiasis is caused by a genetically diverse group of infectious agents. Furthermore, there is no apparent correlation between lineages and clinical manifestation of H. gingivalis (Nadler et al, 2003; Pintore et al, 2017; Olofsson et, 2023). Notably, the only two H. gingivalis sequences available from human cases are those reported in Australia and Germany (Lim et al, 2015; Monoranu et al, 2015), both of which were classified by phylogenetic analysis as belonging to Lineage 1. Unfortunately, a still limited number of sequences are available on public databases, which hampers any hypothesis on a link between zoonotic potential and genetic lineages. The phylogenetic analysis carried out in the frame of this review has highlighted the existence of a putative Lineage 5, including one unpublished H. gingivalissequence identified in Ambrosia beetle (Hyleborus affinis) from Taiwan (Figure 1). The identification of a putative Lineage 5 in an arthopod suggests that the entire genetic diversity of H. gingivalis remains to be discovered, and raises questions about the role of insects in the spread of the parasite. Additional genetic analyses in future cases might reveal any relation between genetic variation, host invasiveness and geographical spread, which would be beneficial not only to prevent equine cases but also for public health.
| Year | Species | Country | Clinical presentation | Diagnosis | Reference |
|---|---|---|---|---|---|
| 1972 | Horse | Egypt | Encephalitis | Post-mortem | Ferris et al, 1972 |
| 1987 | Horse | UK | Encephalitis | Post-mortem, morphological | Blunden et al, 1987 |
| 1990 | Horse | US | Encephalitis, spinal cord lesions | Post-mortem, morphological | Spalding et al, 1990 |
| 1992 | Horse | Scotland | Encephalitis and renal abscess | Post-mortem, morphological | Angus et al, 1992 |
| 1993 | Horse | US | Encephalitis, osteomyelitis | Morphological | Ruggles et al, 1993 |
| 1993 | Horse | US | Encephalitis | Morphological | Trostle et al, 1993 |
| 1993 | Horse | US | Prostitis | Morphological | Dunn et al, 1993 |
| 1995 | Horse | US | Encephalitis | Morphological | Rames et al, 1995 |
| 1998 | Horse | Germany | Osteomyelitis, gingivitis | Morphological | Teifke et al, 1998 |
| 2000 | Horse | US | Encephalitis, nephritis | Morphological | Kinde et al, 2000 |
| 2000 | Grevy's zebra (Equus grevyi) | US | Ocular infection | Morphological | Isaza et al, 2000 |
| 2000 | Horse | Canada | Encephalitis | Post-mortem, morphological | Bröjer et al, 2000 |
| 2001 | Horse | US | Encephalitis | Post-mortem, morphological | Wilkins et al, 2001 |
| 2001 | Horse | US | Encephalitis | Post-mortem, morphological | Johnson et al, 2001 |
| 2001 | Horse | Canada | Encephalitis | Morphological | Pearce et al, 2001 |
| 2004 | Donkey | US | Renal abscess | Morphological | Schmitz and Chaffin, 2004 |
| 2006 | Horse | US | Encephalitis | Post-mortem, morphological | Bryant et al, 2006 |
| 2007 | Horse | Japan | Encephalitis, nephritis | Polymerase chain reaction | Akagami et al, 2007 |
| 2007 | Horse | Brazil | Neurological sign | Post-mortem, histopathology | Vasconcelos et al, 2007 |
| 2008 | Horse | Switzerland | Prostitis | Morphological | Muller et al, 2008 |
| 2008 | Horse | Canada | Encephalitis, mandibular abscess | Morphological | Ferguson et al, 2008 |
| 2011 | Horse | UK | Encephalitis | Post-mortem, morphological | Hermosilla et al, 2011 |
| 2011 | Horse | Canada | Encephalitis | Post-mortem, morphological | Sponseller et al, 2011 |
| 2012 | Horse | Iceland | Encephalitis | Post-mortem, morphological | Eydal et al, 2012 |
| 2012 | Horse | Italy | Encephalitis | Post-mortem, morphological | Di Francesco et al, 2012 |
| 2014 | Horse | South Korea | Encephalitis | Polymerase chain reaction | Jung et al, 2014 |
| 2016 | Horse | Romania | Encephalitis | Polymerase chain reaction, morphological | Taulescu et al, 2016 |
| 2017 | Horse | Italy | Encephalitis | Polymerase chain reaction, morphological | Pintore et al, 2017 |
| 2017 | Horse | Costa Rica | Encephalitis, renal abscess | Post-mortem, histopathology | Berrocal and de Oliveira, 2017 |
| 2017 | Horse | Honduras | Nephritis | Post-mortem, histopathology | Berrocal and de Oliveira, 2017 |
| 2019 | Horse | Portugal | Encephalitis, renal abscess | Post-mortem, histopathology | Noiva et al, 2019 |
| 2020 | Horse | Mexico | Encephalitis | Post-mortem, polymerase chain reaction, histopathology | Avila et al, 2020 |
| 2023 | Horse | US | Anterior uveitis | Post-mortem, histopathology | Pillai et al, 2023 |
| 2023 | Pony | US | Subcutaneous nodules, encephalitis | Polymerase chain reaction, morphological | Baker et al, 2023 |
| 2023 | Horse | Sweden | Encephalitis, nephritis | Post-mortem, polymerase chain reaction, histopathology | Olofsson et al, 2023 |
| 2024 | Horse | Brazil | Arthritis, limb fracture, renal masses | Post-mortem, histopathology | Sousa et al, 2024 |
Life cycle of the parasite
Little is known about the life cycle, mode of infection and pathogenesis of H. gingivalis, but it is believed that the adult female worms reproduce asexually by parthenogenesis. Only females, in association with eggs and immature larvae, have been identified and characterised from tissue samples so far (Lim et al, 2015). Infection routes have been hypothesised to include penetration of compromised skin or mucous membranes, inhalation, transmammary infection of suckling foals and ascending urogenital infection. After host entrance of H. gingivalis, local granuloma formation may be observed, but spread to multiple organ systems occurs more commonly. This is likely via haematogenous and lymphatic routes or through the optic nerve. The contamination of ocular wounds has been speculated as main infection route for H. gingivalis (Rames et al, 1995). Transmammary infection from mare to foal has been also reported in one case (Wilkins et al, 2001). Larvae have been detected in urine samples (Taulescu et al, 2016), and the Musca autumnalis fly has been suggested to act as a carrier (Anderson et al, 1998). Viable Halicephalobus organisms have been isolated from semen, though no transmission via this route has been proven (Kinde et al, 2000). In horses, the reported most common infection sites include the central nervous system, kidneys, maxilla, mandible, regional lymph nodes, eyes and lungs (Onyiche et al, 2017).
Clinical forms
Clinical signs of equine halicephalobosis are related to the host sites involved; neurological signs and renal disease are common to the majority of cases (Bröjer et al, 2000; Bryant et al, 2006; Akagami et al, 2007). Horses with neurological signs have a rapid and progressive neurological deterioration (Keg et al, 1984; Darien et al, 1988; Spalding et al, 1990; Bröjer et al, 2000; Bryant et al, 2006; Akagami et al, 2007). However, clinical forms of infection with H. gingivalis can include also nephritis (Shibahara et al, 2002; Akagami et al, 2007), gingivitis (Teifke et al, 1998), osteomyelitis (Teifke et al, 1998; Ferguson et al, 2008), posthitis (Dunn et al, 1993; Muller et al, 2008), orchitis (Kinde et al, 2000), papillitis (Kinde et al, 2000), retinitis (Kinde et al, 2000) and disseminated disease (Henneke et al, 2014; Pillai et al, 2023). The mean age of previously reported equine halicephalobosis cases was 11.4 years. Similarly to horses, disseminated H. gingivalis infection has been reported in zebras (Isaza et al, 2000) and in humans (Ondrejka et al, 2010). The prognosis of H. gingivalis infection is generally unfavourable, and treatment is usually ineffective in animals with central nervous system or disseminated infection, most likely because of the failure of drugs to cross the blood–brain barrier and/or penetrate the granulomatous lesions. There are only a few reports of successful treatment of this infection in equids; all were localised infections outside the central nervous system (Dunn et al, 1993; Pearce et al, 2001; Schmitz and Chaffin, 2004; Muller et al, 2008). Therefore, parasitic granulomatous disease should be considered as a differential diagnosis in equids with ocular or neurological disease.
Diagnosis
A definitive in vivo diagnosis of H. gingivalis infection is difficult to reach in the absence of accessible granulomatous lesions for biopsies. Therefore, a combination of various methods is commonly required to confirm diagnosis of halicephalobosis in humans and animals (Onyiche et al, 2017). So far, no specific antemortem diagnosis technique is available for diagnosis of the disease in humans and animals. H. gingivalis has never been detected antemortem in bodily fluids (eg cerebrospinal fluid, blood, saliva, joint fluid), with the exception of urine (Kinde et al, 2000). Confirmatory diagnosis relies on either histopathological evaluation of tissues at necropsy or cerebrospinal fluid analysis. Even though a combination of magnetic resonance imaging, haematology and serum biochemical parameters has been evaluated in previous reports, diagnosis is most often based on histopathological evidence of a granulomatous inflammatory process with intralesional ova, rhabditiform nematode larvae and parthenogenic female adults that have characteristic morphological features (in particular, a pointed tail and a reproductive tract with characteristic dorsoflexion of the ovary and ventroflexion of the uterus) (Papadi et al, 2013). Molecular techniques such as polymerase chain reaction have been successful in detecting the parasite DNA in tissues collected at postmortem. Polymerase chain reaction methods of H. gingivalis detection are usually based on the amplification of fragments of rDNA genes; they can be coupled with downstream amplicon sequencing, allowing further molecular investigations, such as molecular typing and phylogenetic analyses (Nadler et al, 2003). However, the type of available matrices – like formalin-fixed paraffin-embedded tissues from histology examinations, which typically carry highly degraded DNA – can hamper the application of molecular methods and decrease their sensitivity (Guyard et al, 2017).
Treatment
Treatment responses in previous cases showed that most affected animals invariably deteriorated, despite anthelmintics (eg ivermectin and benzimidazole) that are routinely administered in most horses (Isaza et al, 2000; Kinde et al, 2000; Ferguson et al, 2008). This was particularly evident in clinical cases involving the central nervous system (Ferguson et al, 2008; Eydal et al, 2012); moreover, the presence of live worms at necropsy supports the idea that common anthelmintic treatment is mostly ineffective. Unsuccessful treatment of H. gingivalis infections may be because of the inability of anthelmintics to cross the blood–brain barrier and penetrate the granulomatous lesions of the central nervous system, or a lack of sensitivity of H. gingivalis to anthelmintic therapies (Trostle et al, 1993). However, few reports in literature describe successful equine halicephalobosis treatment. The first reported case involved preputial granulomas that resolved following systemic treatment with ivermectin and diethylcarbamazine (Dunn et al, 1993). The second case involved a horse with a granuloma over an eye that resolved following surgical debulking, topical ivermectin application and repeated systemic administration of high doses of ivermectin (Pearce et al, 2001). Additionally, unilateral nephrectomy was curative in a donkey with lesions restricted to one kidney (Schmitz and Chaffin, 2004). In cases of localised equine halicephalobosis, a successful treatment can be achieved by oral administration of ivermectin (1.2 mg/kg bodyweight) in intervals of 2 weeks for 3 treatements and excision of the granulomatous lesion (Pearce et al, 2001). Treatment has not been described in human cases, but pharmacokinetic studies suggest that treatment with ivermectin or thiabendazole administered parenterally may not be effective because of poor effect per se and an inability to achieve therapeutic levels in the central nervous system (Fonderie et al, 2012).
Conclusions
As parasitic neurohelminthoses are extremely rare, equine practitioners do not routinely consider H. gingivalis infections in the differential diagnosis of meningoencephalitis. This should be taken into consideration in any rapidly progressing ocular or neurological disease, especially if associated with previous, chronically infected wounds. From a ‘One Health’ perspective, veterinarians should also alert physicians, horse handlers/keepers and other potentially exposed people to the risk of this disease, especially children, who frequently play in potentially contaminated soil and mud. In fact, even though H. gingivalis infection is not contagious, the fact that humans can be infected by contaminated manure makes this parasite a public health concern. To date, there are no specific guidelines for the prevention of equine halicephalobosis. However, the hygiene of the environment and of skin lesions may reduce the risk of infection. A better knowledge of the parasite's biological cycle and contamination routes will be of primary importance to understand the pathogenesis of this infection and to develop in vivo diagnostic methods and an effective therapy. A multidisciplinary approach to problem solving in veterinary medicine is always valuable; from this perspective, the veterinarian's function is of primary importance in detecting possible foci of H. gingivalis contamination and monitoring parasite presence in the environment, particularly through the correct diagnosis of possible cases in horses exhibiting unexplained neurological signs.