

Vitamin E is an essential nutrient in equine diets. It acts as a natural antioxidant, limiting damage from oxidative stress and free radicals. Oxidative damage is associated with toxic cellular effects, which are implicated in the development of a number of diseases, including motor neuron diseases in humans such as amyotrophic lateral sclerosis. In horses, vitamin E supports neuromuscular health. Normal nervous system development is dependent upon adequate vitamin E early in life. Vitamins E and A are the two vitamins that horses cannot produce themselves and must therefore obtain from their diets (National Research Council, 2007).
‘Vitamin E’ was originally a term used to define eight compounds that include four tocopherols and four tocotrienols, each designated as alpha-, beta-, gamma-, or delta- (Table 1). The most bioavailable form of vitamin E for horses is alpha-tocopherol (Finno and Valberg, 2012). Since alpha-tocopherol is also the most potent antioxidant and the only isoform that, when deficient, leads to disease in humans, one proposal suggested renaming vitamin E to include only alpha-tocopherol (Azzi et al, 2023). Thus, for the purposes of this review, the terms alpha-tocopherol and vitamin E will be used interchangeably.
| Tocopherols (saturated) | Tocotrienols (unsaturated) |
|---|---|
| α-tocopherol/vitamin E | α-tocotrienol |
| RRR | |
| RRS | |
| RSS | |
| SSS | |
| RSR | |
| SRS | |
| SRR | |
| SSR | |
| ß-tocopherol | ß-tocotrienol |
| γ-tocopherol | γ-tocotrienol |
| δ-tocopherol | δ-tocotrienol |
Alpha-tocopherol has eight different stereoisomers that are arranged in right or left orientations (Table 1). Naturally occurring alpha-tocopherol (D-alpha-tocopherol) has the R configuration at the three positions of the chromanol ring and is referred to as RRR-alpha-tocopherol.
The main dietary source of vitamin E for horses is fresh green grass. It is important to note that hay alone will not meet dietary vitamin E requirements as it begins to degrade quickly – up to 73% after 12 weeks (National Research Council, 2007) – once it is harvested. Vitamin E is fat-soluble and can be stored in liver, muscle and fatty tissues. Horses naturally draw on these stores as seasonal variations affect the availability of green grass (Mäenpää et al, 1987; 1988). However, modern management practices and worsening drought conditions that limit pasture access interfere with the way horses naturally manage vitamin E, leading to deficiencies and associated health issues.
Vitamin E deficiencies in horses
Although vitamin E is essential in equine diets, deficiency alone does not reliably cause disease. Many horses do not exhibit any clinical signs of disease associated with a vitamin E deficiency (Bookbinder et al, 2019). However, subclinical disease may be occurring at a microscopic level, with oxidised lipopigment (lipofuscin) accumulating in the retina and muscle (Bookbinder et al, 2019). Therefore, any horse with a vitamin E deficiency should be supplemented, whether or not there are clinical signs of disease.
In horses that do develop clinical signs of neuromuscular disease, the development of disease depends on:
Currently, three diseases are known to be associated with vitamin E deficiency in horses.
Equine neuroaxonal dystrophy/equine degenerative myeloencephalopathy
Equine neuroaxonal dystrophy is a spontaneous neurodegenerative disease that develops in foals 6–12 months of age as a result of vitamin E deficiency in the first year of life (Finno et al, 2015), and is one of the top three causes of spinal ataxia in horses (Hales et al, 2021a). Equine degenerative myeloencephalopathy is a more advanced from of equine neuroaxonal dystrophy; the two diseases are clinically indistinguishable.
Clinical signs include symmetric ataxia (which may be more severe in the pelvic limbs), proprioceptive deficits, and an abnormal stance at rest. It is not possible to diagnose equine neuroaxonal dystrophy/equine degenerative myeloencephalopathy based on clinical signs alone, as the disease is indistinguishable from those caused by other neurological diseases. These include cervical vertebral compressive myelopathy, equine protozoal myeloencephalitis or equine herpesvirus-1 myeloencephalopathy (Aleman et al, 2011).
Histologically, equine neuroaxonal dystrophy/equine degenerative myeloencephalopathy is characterised by axonal swellings (spheroids) localised to the caudal medulla oblongata and spinal cord (Finno et al, 2016). Affected horses have significantly lower serum, cerebrospinal fluid and hepatic vitamin E concentrations (Finno et al, 2016). Neurological deficits related to neuroxonal dystrophy often stabilise at 2 to 3 years of age, but do not improve. These horses remain neurologically abnormal for life and are not suitable for performance activities. There is no treatment for equine neuroaxonal dystrophy/equine degenerative myeloencephalopathy (Burns and Finno, 2018). Although a genetic susceptibility to equine neuroaxonal dystrophy/equine degenerative myeloencephalopathy is suspected, the aetiology of the disease remains unknown (Burns and Finno, 2018). There is currently no effective treatment for equine neuroaxonal dystrophy/equine degenerative myeloencephalopathy.
Equine motor neuron disease
Equine motor neuron disease is an acquired neurodegenerative disorder caused by the degenerative loss of motor neurons from the ventral horns of the spinal cord. It is an oxidative disorder that affects neurons supplying highly oxidative type I muscle fibres.
Clinical signs, including weight loss as a result of muscle wasting, muscle fasciculation and extended periods of recumbency, appear after at least 18 months of vitamin E deficiency (de la Rúa-Domènech et al, 1997). However, not all deficient horses develop clinical signs of equine motor neuron disease. Some horses may suffer from subclinical disease, and genetic factors may influence individual susceptibility to disease (Burns and Finno, 2018). Affected horses have low plasma concentrations of vitamin E (de la Rúa-Domènech et al, 1997). Excessive amounts of copper in the diet are a risk factor for developing equine motor neuron disease (Divers et al, 2006).
Diagnosis of equine motor neuron disease requires a muscle biopsy of the sacrocaudlis dorsalis medialis tail head muscle (Divers et al, 1997). In more chronic cases, a biopsy of the spinal accessory nerve may be performed (Jackson et al, 1996). Ocular manifestations include a reticulated pattern at the tapetal–nontapetal junction of the retina, with no evidence of visual impairment (Riis et al, 1999). Vitamin E deficiency is the major risk factor for equine motor neuron disease (Divers et al, 1997). While plasma vitamin E concentrations are often low, low vitamin E concentrations do not always lead to equine motor neuron diease (Divers et al, 2006).
Horses with motor neuron disease may be treated with 5000–7000 IU of alpha-tocopherol daily. Clinical improvement has been reported in 40% of cases within six weeks, with some appearing fully recovered after 3 months.
Vitamin E deficient myopathy
Horses which have clinical signs similar to equine motor neuron disease but lack histological evidence for a conclusive diagnosis may have vitamin E deficient myopathy. It is currently unknown whether vitamin E deficient myopathy is a predecessor to equine motor neuron disease or a separate disease.
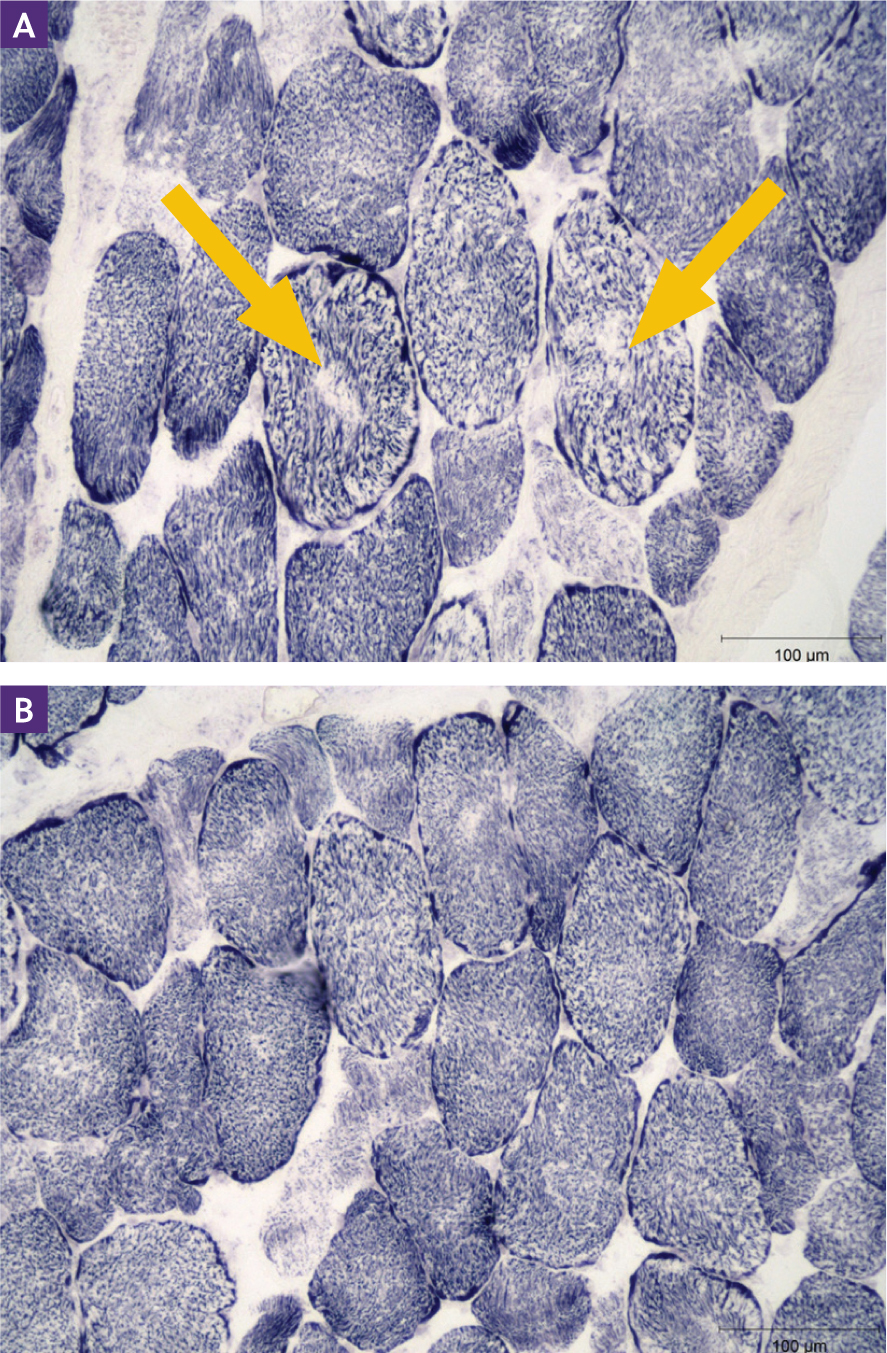
Clinical signs of vitamin E deficient myopathy include generalised weakness and abnormal mitochondrial stains (moth-eaten) in sacrocaudalis dorsalie medialis muscle biopsies (Figure 1). Formalin-fixed muscle biopsies can be used to identify the characteristic abnormalities in mitochondrial staining using an immunohistochemical stain for the enzyme succinate dehydrogenase (Bedford et al, 2013). Fortunately, unlike the previously discussed conditions, horses with vitamin E deficient myopathy can recover completely after vitamin E supplementation (Bedford et al, 2013).
Genetics of vitamin E deficiencies
A genetic component for equine neuroaxonal dystrophy/equine degenerative myeloencephalopathy is likely, based on clusters of case reports involving related horses (Mayhew et al, 1977; Beech and Haskins, 1987; Baumgärtner et al, 1990; Blythe et al, 1991; Finno et al, 2011). Other studies have provided further support for a genetic susceptibility for equine neuroaxonal dystrophy/equine degenerative myeloencephalopathy. In one longitudinal study of 14 foals (10 from healthy dams and sires, four from dams with equine neuroaxonal dystrophy/equine degenerative myeloencephalopathy) maintained on a vitamin E-deficient diet from birth until eight months of age, only the four genetically susceptible foals developed clinical and histological evidence of equine neuroaxonal dystrophy/equine degenerative myeloencephalopathy (Finno et al, 2015). Cases of equine neuroaxonal dystrophy/equine degenerative myeloencephalopathy have been reported across breeds (Table 2), but the cause of the disease may not be the same in each breed.
| Breed | Reference(s) |
|---|---|
| American Paint Horse | Blythe and Craig, 1992 |
| American Quarter Horse | Gandini et al, 2004; Aleman et al, 2011 |
| Appaloosa | Blythe et al, 1991 |
| Arabian | Sisó et al, 2003 |
| Haflinger | Baumgärtner et al, 1990 |
| Lusitano | Finno et al, 2011 |
| Mixed breeds | Mayhew et al, 1977; Dill et al, 1989 |
| Mongolian Horse | Liu et al, 1983 |
| Morgan Horse | Beech and Haskins, 1987 |
| Norwegian Fjord Horse | Blythe and Craig, 1992 |
| Paso Fino | Mayhew et al, 1987 |
| Standardbred | Mayhew et al, 1987 |
| Tennessee Walking Horse | Blythe and Craig, 1992 |
| Thoroughbred | Mayhew et al, 1978; Cummings et al, 1995 |
| Warmblood | Finno et al, 2017 |
| Welsh Pony | Blythe and Craig, 1992 |
Various modes of inheritance have been proposed for equine neuroaxonal dystrophy/equine degenerative myeloencephalopathy. To date, research supports an autosomal dominant with incomplete penetrance or polygenic mode of inheritance; a high heritability of 0.70 was established in one population of Quarter Horses (Finno et al, 2013).
Comparatively, equine neuroaxonal dystrophy/equine degenerative myeloencephalopathy clinically and histologically resembles ataxia with vitamin E deficiency in humans, which is caused by mutations in the alpha-tocopherol transfer protein gene (Gotoda et al, 1995; Yokota et al, 1997). Despite the phenotypical similarities, the same gene was not responsible for equine neuroaxonal dystrophy/equine degenerative myeloencephalopathy in a population of Quarter Horses (Finno et al, 2013). Hales et al (2020) found that a 2.5 Mb region on equine chromosome 7 was associated with equine neuroaxonal dystrophy/equine degenerative myeloencephalopathy in a strictly phenotyped population of Quarter Horses. This region contained three variants identified in the caytaxin gene, which is associated with Cayman Ataxia and ataxic/dystonic phenotypes in mouse models (Hales et al, 2020). It was determined that they were not concordant with equine neuroaxonal dystrophy/equine degenerative myeloencephalopathy.
Genome-wide association studies have been complicated by population stratification because of relatedness, multiple breed study designs, small sample size, insufficient marker density and unknown environmental factors.
Vitamin E testing
Vitamin E concentrations can be measured in serum or plasma. While concentrations are highly correlated between serum and plasma samples, it is recommended to remain consistent when resampling the same horse (ie either always use serum or always use plasma) (Hales et al, 2021b). Samples should be refrigerated upright for up to 72 hours. If longer storage is needed, the serum or plasma should be separated. Samples should also be protected from light. Vitamin E testing evaluates the concentration of alpha-tocopherol in the sample. Normal reference range concentrations of alpha-tocopherol in horse plasma and serum are (Vanschandevijl et al, 2008):
While these reference ranges remain suitable, more recent studies have demonstrated that horses grazing on pasture for at least 12 hours/day typically have serum vitamin E concentrations between 3–6 µg/mL (Habib et al, 2021). Therefore, it is recommended to target these concentrations during supplementation.
The National Research Council (2007) daily recommendations for vitamin E in horses are 1–2 IU/kg bodyweight. This equates to approximately 500 IU of vitamin E per day for a 500 kg horse that is in light work. For horses in harder work, this might increase to up to 1000 IU daily.
It is important to note that the National Research Council recommendations were established based on the bioavailability of the synthetic (all-rac) formulation of vitamin E. When using the more bioavailable formulations, such as the water-dispersible micellised form of alpha-tocopherol, the bioavailability approaches 2x that of the synthetic product (Pagan et al, 2005).
Baseline vitamin E concentrations vary widely in healthy horses. Factors to consider in the evaluation of blood alpha-tocopherol levels include age (foals have significantly lower levels than adults), diet, when the sample was taken and how it was stored (Finno and Valberg, 2012). Horses with vitamin E deficiency exhibit larger fluctuations in serum alpha-tocopherol than horses that are not deficient, possibly caused by recirculation of alpha-tocopherol between the plasma and liver (Vanschandevijl et al, 2008).
Phosphorylated neurofilament heavy subunit pNF-H testing for equine neuroaxonal dystrophy/equine degenerative myeloencephalopathy
Measurement of phosphorylated neurofilament heavy subunit, a biomarker of axon damage, in serum and/or cerebrospinal fluid by enzyme-linked immunosorbent assay capture is the first supportive antemortem diagnostic test available for equine neuroaxonal dystrophy/equine degenerative myeloencephalopathy. Diagnosis otherwise requires postmortem evaluation of the brainstem and spinal cord.
The phosphorylated neurofilament heavy subunit test has higher sensitivity in horses younger than five years of age as compared to older horses (Edwards et al, 2022) and it is important to know a horse's protozoal myeloencephalitis status before running the phosphorylated neurofilament heavy subunit biomarker assay. If the horse is negative for protozoal myeloencephalitis, a diagnosis of equine neuroaxonal dystrophy/equine degenerative myeloencephalopathy or cervical vertebral compressive myelopathy is possible, and may be further refined with the phosphorylated neurofilament heavy subunit test. Diagnostics for protazoal myeloencephalitis should ideally be run on the same cerebrospinal fluid sample and protazoal myeloencephalitis should be excluded before proceeding with the phosphorylated neurofilament heavy subunit testing (Edwards et al, 2022).
Supplementing with vitamin E
It is important to obtain baseline vitamin E values before supplementation as these can vary widely among individuals (Craig et al, 1989) and are necessary to properly adjust levels of dietary vitamin E to account for seasonal and/or dietary changes. It should be noted that commercial feed products, such as grains, are fortified with vitamins including vitamin E, and this should be accounted for when determining appropriate supplementation levels.
Horses should be fed the natural RRR-alpha-tocopherol formulation, as opposed to synthetic (all-rac-alpha-tocopherol), especially if they have been diagnosed with motor neuron disease, equine neuroaxonal dystrophy/equine degenerative myeloencephalopathy or vitamin E deficient myopathy (Mustacich et al, 2007a). There is currently no evidence that alpha-tocopherol supplementation in excess of the 2007 National Research Council-recommended dose has additional therapeutic benefits for horses with neurological deficits (Lekeux and Kirschvink, 2009).
Unlike other fat-soluble vitamins, toxic levels of vitamin E do not accumulate in the body (Traber, 2013). Although excessive supplementation can increase vitamin E concentrations in blood and tissues, excess alpha-tocoperol is metabolised and/or excreted in the urine (Mustacich et al, 2007b). Potential toxicity from high dose-supplementation of vitamin E in horses is minimal. However, levels above the recommended upper safe diet concentration of 20 IU/kg bodyweight have been reported to lead to coagulopathy and impaired bone mineralisation in some cases (National Research Council, 2007). Supplementation at ten times the National Research Council recommendation interferes with normal absorption of certain nutrients (Williams and Carlucci, 2006).
It should also be noted that the metabolism and absorption of vitamin E occurs along shared pathways with other biological processes. For example, vitamin E has the same absorption pathway as beta carotene (vitamin A), so oversupplementation of vitamin E can decrease beta carotene levels (Williams and Carlucci, 2006). Similarly, vitamin E is metabolised through the cytochrome P450 system, which is the same system that processes many therapeutic drugs. It is important to exercise caution when supplementing vitamin E for horses that are being treated with certain medications, as high doses of alpha-tocopherol can lead to increased drug bioavailability and associated adverse effects (Kliewer et al, 2002; Blatt et al, 2004).
Prevention is key
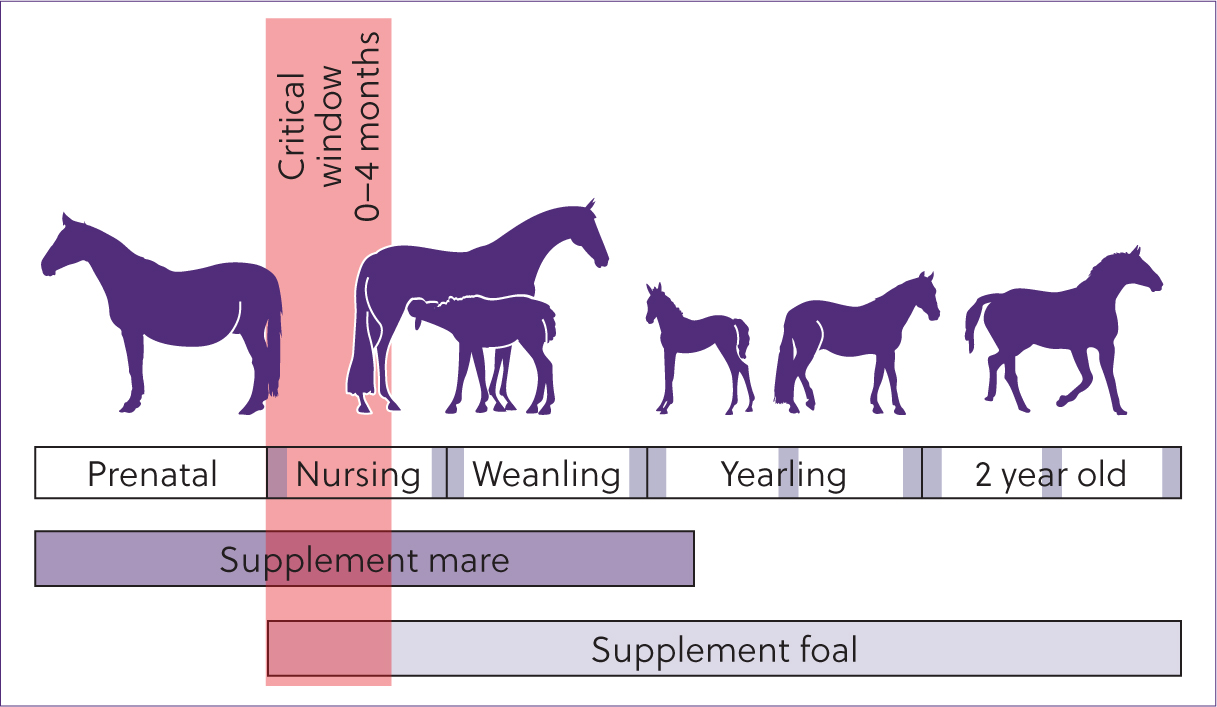
Eliminating the risk of vitamin E deficiencies in horses begins early in life. Ideally, pregnant mares, foals, weanlings, yearlings and 2-year-old horses should be maintained on lush green pastures to ensure adequate vitamin E intake. In young horses, this protects the developing central nervous system from neurodegeneration (Burns and Finno, 2018). In the absence of adequate pasture, management should follow that which is outlined in Figure 3 (Finno et al, 2015).
In the author's experience, horses as young as one to two months of age can show clinical signs of vitamin E deficiencies. If at all possible on high risk breeding farms, foals should have neurological examinations at one and six months of age. For early disease detection, additional examinations should be conducted every 6 months until the horse reaches 4–5 years of age. Ideally, a foal's serum alpha-tocopherol level should be measured in the first week of life. This is when the largest difference between foals that experience normal neurological development and those that develop equine neuroaxonal dystrophy/equine degenerative myeloencephalopathy is observed (Finno et al, 2015). If this is not feasible, the foal's serum alpha-tocopherol level should at least be measured within the first 4 months of life. This is the only time in which a difference exists between the two groups (Finno et al, 2015).
Conclusions
Vitamin E plays an important role in equine diets. As regions increasingly experience drought conditions, access to vitamin E through fresh grass is declining. Ongoing research into the genetic cause(s) of diseases associated with vitamin E deficiencies will provide additional information to identify susceptible individuals and develop appropriate treatment and management plans. Further research into antemortem detection assays may help provide earlier diagnosis than currently available methods.