

Sand enteropathy refers to pathology of the intestines associated with the accumulation of sand. In horses, the build-up of sand occurs primarily in the large colon. The condition is common and affects horses in locations where sand occurs in the environment, with reports from geographical locations worldwide. For example, cases have been reported in North America (Bertone et al, 1988; Keppie et al, 2008), Europe (Husted et al, 2005; Graubner et al, 2017; Loschelder and Gehlen, 2017; Niinistö et al, 2019), Australia (Granot et al, 2008), Brazil (Alonso et al, 2020), Israel (Granot et al, 2008) and the United Arab Emirates (Morales-Briceño, 2022).
There is no sex predilection in horses who experience this gastrointestinal disease (Keppie et al, 2008; Hart et al, 2013; Kilcoyne et al, 2017). Some breeds, such as Quarter Horses (Keppie et al, 2008; Hart et al, 2013; Kilcoyne et al, 2017), Shetland ponies (Graubner et al, 2017), Miniature horses (Granot et al, 2008; Keppie et al, 2008; Hart et al, 2013) and Finnhorses, (Ruohoniemi et al, 2001; Kaikkonen et al, 2016) are overrepresented in the literature. However, this could also be a reflection on horse populations in areas where sand is more common in the environment. Thoroughbreds, which are represented worldwide, are rarely affected by sand enteropathy (Granot et al, 2008; Hart et al, 2013; Kilcoyne et al, 2017); this might be related to the more controlled management of this breed compared to the others.
Horses that are considered greedy and those which have lower status in the herd hierarchy are at higher risk of sand accumulation, most likely because they tend to eat from the ground when less food is present, leading to an increased risk of ingesting sand (Niinistö et al, 2019). Logically, sandy soil is a risk factor for sand accumulation (Sanchez, 2018). However, the relationship between access to sand and sand enteropathy is not as clear cut as sand simply being present in the environment. For example, a study involving Icelandic horses in Denmark assessing the effect of different types of soils on sand faecal output failed to find a significant difference between soil types when this variable was tested as the main effect (Husted et al, 2005). However, the same study showed that offering food directly from the ground in paddocks with no, or sparse, grass cover was associated with an increased risk of faecal sand excretion (Husted et al, 2005). Furthermore, when compared to paddocks with no grass, not offering additional food in sparse grass paddocks was also considered a risk factor for sand excretion, because horses kept grazing until the grass was very short, increasing the risk of unintentionally ingesting sand (Husted et al, 2005). Overall, the study concluded that the risk of sand intake was multifactorial and influenced by soil type, pasture quality and feeding practice (Husted et al, 2005).
Despite some of the risk factors being known, the reason why sand accumulates within the gastrointestinal tract of some horses is not clear. Certain horses, especially foals (Specht and Colahan, 1988; Siwińska et al, 2019), have been reported to deliberately ingest sand while on pasture, although the motives behind this behaviour are not clear (McGreevy et al, 2001). Other horses accidentally eat sand while grazing or eating on pasture (Sanchez, 2018). However, ingestion of sand does not always lead to its accumulation in the large colon, as some horses are able to clear ingested sand while others are not (Sanchez, 2018). Veterinary understanding of why this variation between horses occurs is currently poorly understood.
Diagnosis
Clinical signs associated with sand accumulation can be varied, nonspecific and often overlap with other presentations of gastrointestinal diseases. One of the most common presentations is acute colic (Granot et al, 2008; Hart et al, 2013; Kaikkonen et al, 2016; Kilcoyne et al, 2017; Niinistö et al, 2019). This usually occurs when the accumulated sand causes either a partial or complete obstruction of the large colon, sometimes combined with gas distension of the colon proximal to the obstruction, leading to clinical signs of colic. In some cases, the impaction can be palpated during a transrectal examination and faeces with sand can be retrieved from the rectum (Figure 1). It has been reported that a ‘seashell’ sound can be auscultated when the stethoscope is placed on the ventral abdomen of a horse with sand accumulation (Ragle et al, 1989a; Niinistö and Sykes, 2022). However, this test is considered to have a low sensitivity, leading to many false negatives (Ragle et al, 1989a; Niinistö and Sykes, 2022). Moreover, a large accumulation of sand within the large colon will most likely not produce any sound, as the accumulation does not move. On the other hand, the presence of a seashell sound might be correlated with a small amount of sand present, which might not be clinically significant, also leading to a false positive. Overall, the test appears to have very little use in general practice.

Another common presentation is intermittent chronic diarrhoea, which can be concurrent with weight loss. However, there does not appear to be a direct relationship between the amount of sand accumulated in the colon and the presence of diarrhoea (Niinistö et al, 2019). Diarrhoea was the most common clinical sign reported in a study of 358 horses with radiographic evidence of sand accumulation, with 55.9% of the horses afflicted; this suggests that even a small quantity of sand can likely induce diarrhoea (Niinistö et al, 2019). The same study showed an association between reported colic or poor performance and the size of radiograph sand accumulation, with a larger accumulation more likely to be associated with those symptoms. This lead to the conclusion that sand enteropathy might play a role in poor performance cases and should be considered in the differential diagnoses, especially if poor performance is associated with episodes of colic and/or diarrhoea (Niinistö et al, 2019). Moreover, because many clinical signs of sand enteropathy are similar to those associated with gastric ulcers, sand enteropathy should be included as a differential diagnosis for equine gastric ulcer syndrome (Niinistö and Sykes, 2022). Interestingly, sand has been reported to have a protective role in the development of equine glandular gastric disease in a population of Finnish horses. However, this could be explained by the longer time these horses spent grazing, which might reduce the risk of glandular gastric disease while increasing the risk of ingesting sand (Mönki et al, 2016).
Horses may accumulate sand without any clinical signs (Kendall et al, 2008; Kaikkonen et al, 2016). No study has correlated the amount of sand present in the gastrointestinal tract with clinical signs. Clinical signs may relate to the size of the horse relative to the amount of sand and individual predisposition, especially considering that some horses accumulate sand while others do not (Bertone et al, 1988; Keppie et al, 2008; Hart et al, 2013).
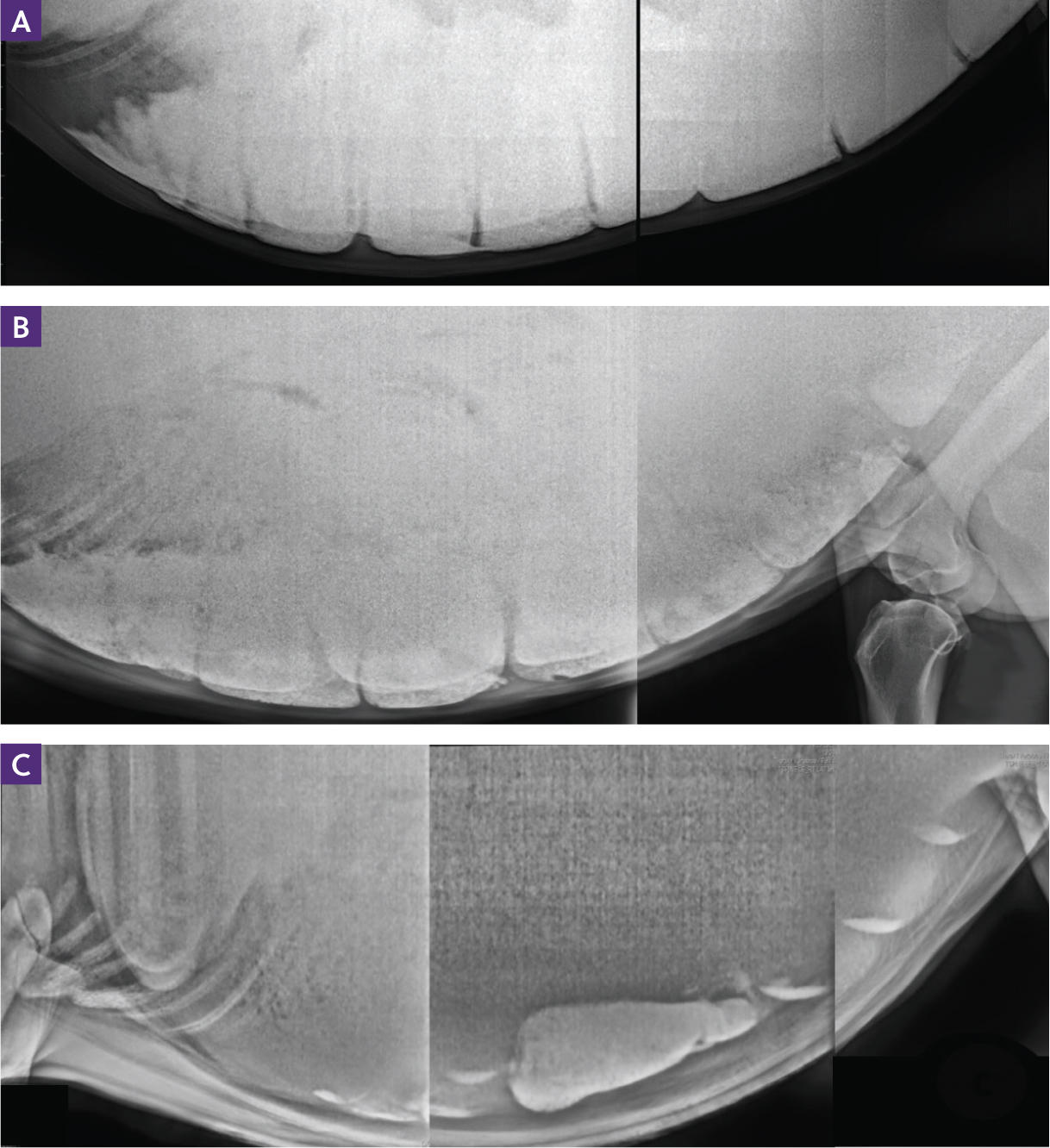
The best method to identify sand enteropathy is a radiographic study of the ventral abdomen, which can reveal the presence of sedimented sand within the large colon (Figure 2). Usually, depending on the size of the horse and the plate, four or five latero–lateral projections are needed to cover the entire ventral abdomen, although Kendall et al (2008) suggested that two or three projections of the most cranioventral part of the abdomen are sufficient to reveal the presence or absence of sand accumulation in an average size horse (450 kg). Repeated radiographic examination of the abdomen during and following treatment are also considered an important tool to monitor the resolution of sand accumulation (Ruohoniemi et al, 2001; Hart et al, 2013) (Figure 3). However, quantifying the amount and the exact location of the sand can prove challenging.
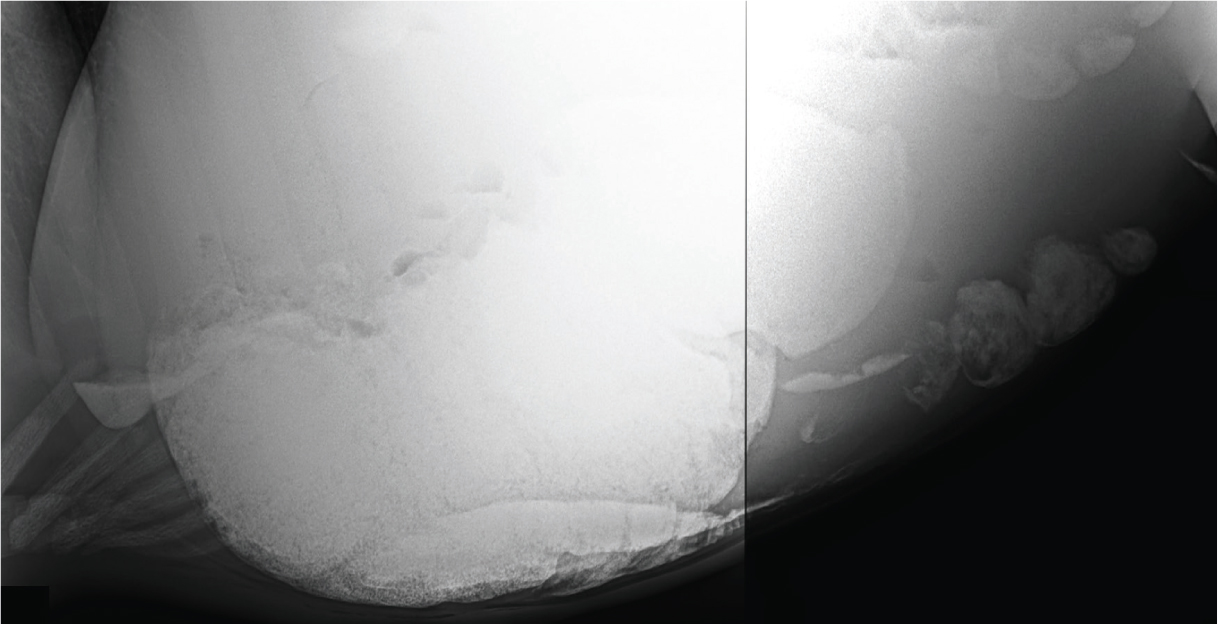
Several subjective and objective methods have been described to evaluate the amount of sand, chiefly by evaluating variables on the radiographs. The variables include the absolute, or relative to the rib, height and length of the accumulations (Korolainen and Ruohoniemi, 2002; Kendall et al, 2008; Keppie et al, 2008), the number of accumulations (Keppie et al, 2008), their location(s) (Keppie et al, 2008), the area of the accumulation (Niinistö et al, 2014; Kaikonnen et al, 2016; Kilcoyne et al, 2017) and the opacity of sand accumulation relative to the rib (Keppie et al, 2008). Some of these parameters are considered alone or simultaneously, and grading systems have been proposed based on these radiographic findings (Korolainen and Ruohoniemi, 2002; Keppie et al, 2008). Unfortunately, because of the two-dimensional nature of the radiographic studies and possible magnification errors resulting from the location of the accumulations relative to the cassette position, it is unlikely that any of these methods accurately quantify the amount of sand present. This may explain why the amount of sand necessary to cause clinical signs has not been determined. Nevertheless, in attempting to characterise the amount of sand with clinical signs, Niinistö et al (2014) considered a sand impaction resolved when the area of sand visible radiographically was <25 cm2 in horses heavier than 300 kg.
Ultrasound examination of the ventral portion of the abdomen along the midline has been identified as a useful complementary tool to identify sand accumulation, but it does not give information regarding the amount of sand present. This method of clinical assessment has been reported to have an 87.5% specificity and sensitivity when compared with radiography (Korolainen and Ruohoniemi, 2002). On ultrasound imaging, the accumulation of sand appears hyperechoic with an acoustic shadow, and is often associated with poor or no motility of the intestine in that area and a flat appearance of the mucosa (Korolainen and Ruohoniemi, 2002). Typically, the colon appears lying on the ventral abdominal wall, and compression of abdominal fat can also sometimes be observed as a result of the weight of the accumulated sand in the colon (Korolainen and Ruohoniemi, 2002). Although the imaging provided by ultrasonography cannot replace radiography, it is a useful adjunct diagnostic and has been shown to be a reliable method of monitoring the resolution of sand accumulation, especially when radiography and ultrasonography are performed at the first examination (Korolainen and Ruohoniemi, 2002). Ultrasonography is easily performed in an ambulatory setting and carries no radiation risk (Korolainen and Ruohoniemi, 2002).
The faecal glove sedimentation test is an easy and inexpensive diagnostic tool that consists of mixing faeces with water in a rectal glove and letting the solution settle for 5–10 minutes; if sand is present, it will form a sediment at the fingertips of the glove (Figure 4). Although this method is frequently used to identify horses with sand enteropathy, caution should be made in its interpretation. This is because a positive test might only mean ingestion of sand without actual accumulation, while a negative one does not exclude sand enteropathy from the differential diagnosis (Filgueiras et al, 2009). However, given the high sensitivity (83%) and positive predictive value (90%) of the test in a population of horses presenting with clinical signs of colic and a high prevalence of sand enteropathy, treatment based on a positive faecal glove sedimentation test in a similar population could be justified, especially if other diagnostic methods are not available (Hukkinen, 2015; Niinistö and Sykes, 2022). Moreover, the test could be useful in monitoring sand clearance during treatment and could be combined with ultrasonography and radiography when the accumulation does not resolve or sand is not detected in the faeces (Korolainen and Ruohoniemi, 2002).

Treatment
Once sand accumulation has been identified, treatment will depend mainly on the clinical presentation of the horse. Animals with clinical signs of moderate to severe colic should first be treated to manage and control pain, and resolve any possible abnormalities related to the colic episode, such as dehydration, electrolyte imbalances and gas distension. Details on resolving these abnormalities are outside the scope of this article.
Medical treatment is indicated once the acute phase is resolved and in cases where the accumulation presents without clinical signs of colic. Horses that present with concurrent pathologies causing colic symptoms (eg large colon displacement, small intestinal colic) should be treated in order to resolve the primary issue before addressing the sand accumulation. In cases where the primary issue requires surgery, surgical treatment of sand accumulation should be performed as well. The main products described in the literature are psyllium husk, which creates a gel when hydrated, and magnesium sulphate, an osmotic laxative.
The combination of psyllium (1 g/kg bodyweight) and magnesium sulphate (1 g/kg bodyweight) mixed with 15 ml/kg body weight of water administered via nasogastric tube once daily is superior to the administration of psyllium (1 g/kg bodyweight) or magnesium sulphate (1 g/kg bodyweight) alone mixed with 15 ml/kg bodyweight of water. Niinistö et al (2014) found that 75% of horses cleared the sand after 4 days of combination treatment, compared to only 25% and 16% when psyllium or magnesium sulphate were used alone, respectively. When the combination of psyllium and magnesium sulphate was compared to a control group that did not have access to sand, the sand clearance was significantly better in the treatment group (Niinistö et al, 2018). However, around 20% of control horses cleared the sand accumulation; this was a similar result in response to monotherapy in the study by Niinistö et al (2014), leading to the speculation that removing horses from having access to sand might be as beneficial as administering psyllium or magnesium sulphate, and could be effective in treating sand enteropathy in some cases (Niinistö et al, 2018). The combination of psyllium and magnesium sulphate for 3–7 days was also compared with oral administration of psyllium for 10 days and a single nasogastric administration of the combination followed by 10 days of oral psyllium (Kaikkonen et al, 2016). This showed a greater sand clearance with the nasogastric administration of the combination for 3–7 days (53%) with only 21–24% of horses resolving the sand accumulation in other two treatment groups (Kaikkonen et al, 2016). Therefore, despite the oral administration of psyllium being advocated as good practice for treating and preventing sand accumulation, its effect is comparable to avoiding sand exposure. Moreover, a study by Hassel et al (2020), which evaluated the effect of a product that combines psyllium with probiotics and prebiotics administered orally for 35 days, showed no difference in sand clearance when compared with an untreated group. Another study compared the use of psyllium (1 g/kg bodyweight) with carboxymethylcellulose (1 g/kg bodyweight) and observed no difference in sand clearance after a single administration, suggesting again that monotherapy has little effect on sand clearance (Alonso et al, 2020). Because administration of psyllium and magnesium sulphate can cause some mild discomfort and distension of the stomach secondary to the swelling of the psyllium, administering a dose of flunixin meglumine (1.1 mg/kg intravenously) and fasting the horse for at least 4 hours before giving the combination has been suggested (Niinistö and Sykes, 2022). Possible complications reported after the administration of psyllium include stomach rupture (Bergstrom et al, 2018) and magnesium toxicosis following magnesium sulphate treatment (Henninger and Horst, 1997). Withholding food for >4 hours before administering the psyllium may avoid possible stomach rupture (Niinistö and Sykes, 2022). The use of magnesium sulphate should be avoided in horses with renal issues, and toxicosis should be treated with intravenous fluid with calcium supplementation (Henninger and Horst, 1997). Evaluating the magnesium level in the blood could also be a useful test to perform before administering the laxative, although this requires access to a laboratory. From the author's experience, decreasing the amount of magnesium administered (0.5 g/kg) could also be considered. Overall, medical management of sand enteropathy carries a good prognosis, with success rates of 86–94% reported (Hart et al, 2013; Kilcoyne et al, 2017).
Cases where the pain or sand impaction cannot be managed medically, or the clinical status of the horse deteriorates, should be referred for an exploratory laparotomy. Surgical management of sand enteropathy is required in around 14–24% of cases (Hart et al, 2013; Kilcoyne et al, 2017), but this is not directly correlated with the amount of sand observed during the radiographic study (Kilcoyne et al, 2017). However, the accumulation of gas may also be a predictor for surgery. In one study of 153 horses with sand accumulated in the large colon, an increased accumulation of gas on radiographs and transrectal palpation of impaction or intestinal gas distension increased the likelihood of surgery (Kilcoyne et al, 2017). Short-term survival for surgically managed sand enteropathy has been reported as 55–94% (Ragle et al, 1989b; Granot et al, 2008; Hart et al, 2013; Kilcoyne et al, 2017), and the presence of concurrent gastrointestinal pathologies, such as displacement or volvulus, reportedly carries a poorer prognosis (Hart et al, 2013). These results are comparable to short-term survival for colic surgery in previous studies (van Loon et al, 2020; Spadari et al, 2023) and large colon impaction treated surgically (83%; Spadari et al, 2023).
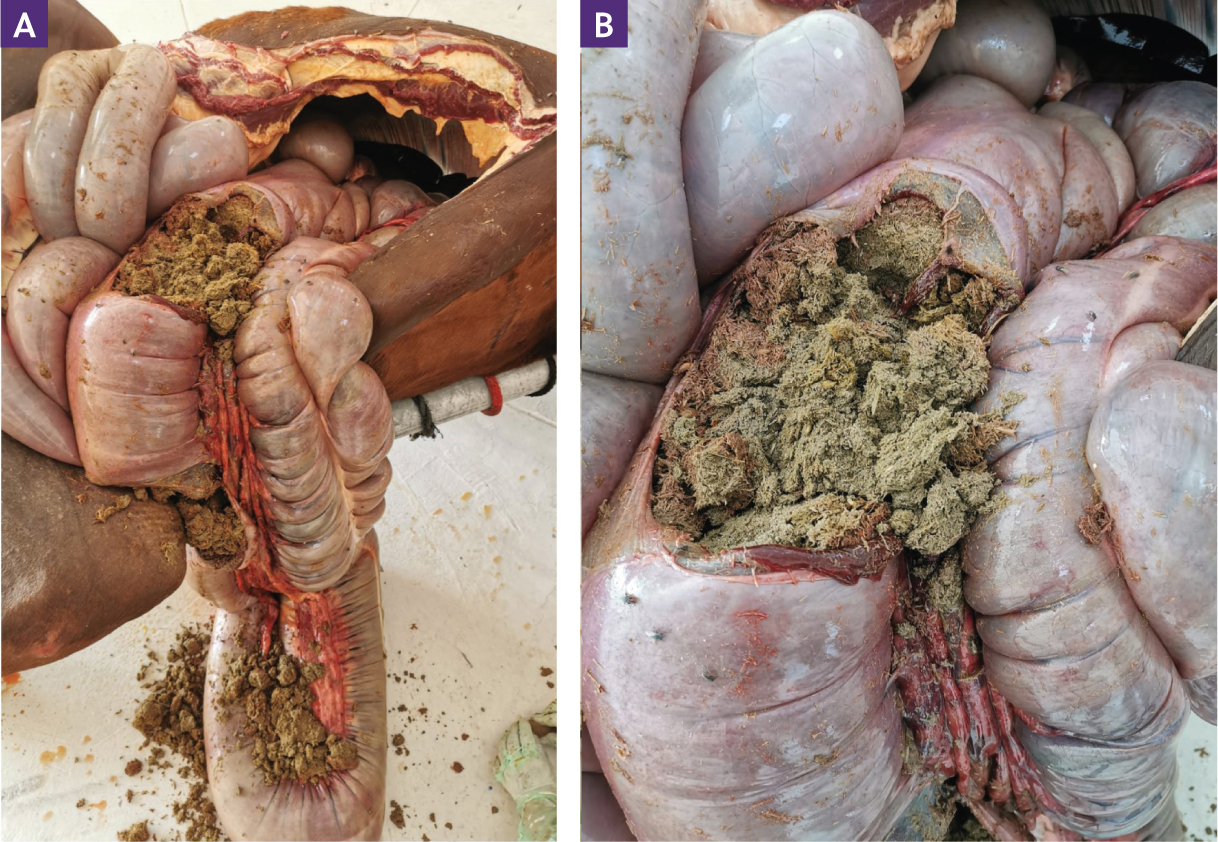
During surgery, the large colon is carefully exteriorised, and any sand evacuated through an enterotomy. Extreme care must be exercised when manipulating the intestine with sand accumulation; the risk of rupture is extremely high because of the fragile intestinal wall, especially in chronic cases (Specht and Colahan, 1988; Ragle et al, 1989b; Granot et al, 2008). The weight of the accumulated sand can also present a challenge for the surgeon in exteriorising the colon. In some cases, tilting the horse laterally allows partial evacuation of the colon, thus reducing its weight and making it easier to handle (Ragle et al, 1989b). Tears and ruptures of the large colon have been reported as a result of surgery (Granot et al, 2008; Kilcoyne et al, 2017) (Figure 5).
Prevention
Studies regarding preventing sand accumulation are lacking. Daily administration of oral psyllium is often recommended, but its efficacy has been questioned (Kaikkonen et al, 2016; Hassel et al, 2020). However, most of the horses evaluated in the studies assessing oral psyllium alone were treated when large sand impactions were already present. As such, it is difficult to make assumptions regarding the efficacy of oral psyllium in preventing accumulation. There is a need for further research in this area.
As avoiding sand exposure appears to be the only proven and reasonable method to prevent sand ingestion and accumulation, changes in the management of susceptible horses should be implemented. Placing rubber mats (which must be cleaned daily) where the horses are fed can reduce the amount of sand ingested to prevent any sand accumulation (Niinistö and Sykes, 2022). Providing adequate and additional food (according to the type and medical condition of the horse) when horses are in paddocks is a protective factor (Husted et al, 2005) in preventing sand accumulation. As animals lower in the hierarchy were more prone to sand accumulation, separating them during feeding might aid in preventing sand enteropathy (Niinistö et al, 2019). For horses kept in sand paddocks, in countries such as the United Arab Emirates, feeding hay and hard feed off the ground in racks designed to prevent spillage into the sand with rubber mats underneath can also aid in reducing sand intake.
Conclusions
Sand enteropathy is a common and worldwide gastrointestinal issue that can affect any breed of horse. Given that the clinical findings can easily overlap with other gastrointestinal diseases, including equine gastric ulcer syndrome, sand enteropathy should always be considered as a differential diagnosis. Radiography is the gold standard for diagnosing the presence of sand accumulation. However, evaluating the amount and clinical significance of the accumulation is often challenging. Medical treatment is often successful, and the use of a combination of psyllium and magnesium sulphate is recommended. However, some cases might require surgical evacuation of the sand accumulation. Prevention of sand accumulation can represent a challenge, especially where horses are kept on sand paddocks. Further study is needed to better understand why some animals are more prone to showing clinical signs following ingestion while others appear unaffected.