

This is the second part of a two-part article on post-foaling colic in the broodmare. These cases often present a diagnostic challenge, particularly out in the field, and rapid triage and diagnosis are important to ensure the best possible outcome for both mare and foal. Foaling itself involves substantial forces that are sustained by maternal tissues, putting the mare at increased risk of haemorrhage and rupture. As mentioned in part 1 (Bozorgamanesh, 20224), for simplicity, the author divides these conditions into conditions of the gastrointestinal tract, and those of the genitourinary and reproductive tracts (Table 1). This two-part article describes diagnostic essentials for first-opinion practitioners to identify key features of some of the most common differential diagnoses for colic in the post-foaling mare. The general approach to the post foaling colic has been covered in part 1, as well as discussion of conditions of the gastrointestinal tract. Part 2 will focus on conditions of the genitourinary and reproductive tracts, covering conditions with non-specific colic signs where the diagnosis is not immediately apparent on examination, such as uterine prolapse.
| Conditions of the gastrointestinal tract | Conditions of the genitourinary and reproductive tracts |
|---|---|
|
|
|
Periparturient haemorrhage
Periparturient haemorrhage has been estimated to affect 2–3% of broodmares and account for 40% of periparturient deaths (Frazer, 2003a; Arnold et al, 2008). Haemorrhage may occur prepartum but is most common within 48 hours post-foaling (Pascoe, 1979; Rossdale, 1994; Arnold et al, 2008). The uterine artery is the most common origin of the haemorrhage, resulting in haematoma formation if contained within the broad ligament or haemoabdomen if not. Other vessels that may be affected include the ovarian, external iliac and vaginal arteries (Rooney, 1964; Pascoe, 1979; Rossdale, 1994; Arnold et al, 2008; Williams and Bryant, 2012). Mares can also haemorrhage into their uterus or vagina, and haematomas can also form within the wall of the uterus or vagina. Increased risk of periparturient haemorrhage is thought to be associated with increased parity, age and following dystocia or more traumatic foaling (Turner, 2007). Postmortem histological evaluation of ruptured uterine arteries has revealed evidence of degenerative changes of the internal elastic membrane and fibrosis of the intima, which are likely associated with parity and age (Rooney, 1964).
Clinical signs of periparturient haemorrhage are most commonly abdominal pain, although these can vary from lethargy to cardiovascular shock. Typically, mares show signs of moderate discomfort including agitation, pacing, pawing, sweating, muscle fasciculations and flank watching, and they often will lay down and groan (Rooney, 1964; Frazer, 2003a; 2003b; Arnold et al, 2008). More severe signs of pain are often associated with broad ligament haematomas where the build of pressure further exacerbates the discomfort. As signs are non-specific and there are many other potential causes of colic in post-foaling mares, diagnosis can be challenging. More invasive diagnostic procedures have the potential to cause increased agitation of the mare, which may precipitate uncontrolled haemorrhage. As such, the author recommends starting with physical examination, transabdominal ultrasound examination and blood work analysis. Ideally, rectal palpation and transrectal ultrasound examination should be avoided in cases of periparturient haemorrhage until the mare has stabilised (Frazer, 2003a).
It is important to remember that mares can show a variety of signs depending on the duration and severity of haemorrhage before examination. Mares with periparturient haemorrhage will often have pale mucous membranes (Figure 1), cold extremities and be tachycardic and sweaty. This is in contrast to mares with a uterine tear or large colon volvulus, whose mucous membranes tend to be either bright red or purple as a result of endotoxaemia. Mares that are haemorrhaging into their uterus or vagina often haemorrhage externally from their vulva, although the post-foaling uterus is very large and pendulous and may become distended with blood and extend cranially in the ventral abdomen. Bleeding into the vaginal wall leads to peri-vulval swelling that can be visualised externally. Haematological and biochemical abnormalities may not be indicative of haemorrhage in the acute stages; however, these are more supportive of the diagnosis in advanced stages after compensatory mechanisms, such as splenic contraction, have been exhausted (Rossdale, 1994; Crabtree, 2012). Hyperlactataemia is often present, depending on the degree of hypoperfusion, and is a useful stable-side test to help evaluate the status of these mares and trends in their condition. Hypoalbuminaemia and/or hypoproteinemia is often noted earlier than anaemia, which may take up to 12 hours to be evident on blood work. Other abnormalities include azotaemia and coagulation deficiencies (Rossdale, 1994; Frazer et al, 2003a; Arnold et al, 2008).

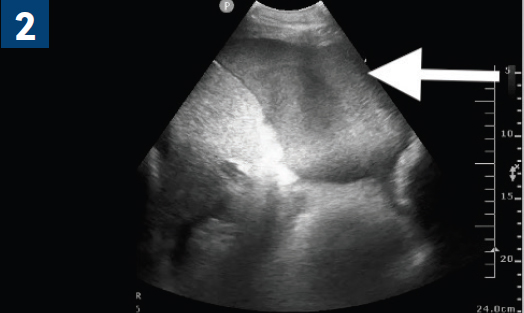
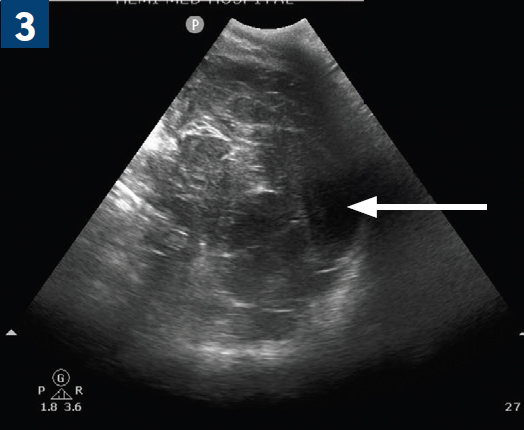
Transabdominal ultrasound examination is an essential part of diagnosis and can be used to identify haemoabdomen andhaematomas within the abdomen, broad ligament or elsewhere. Haemoabdomen is characterised by free abdominal fluid with a homogenous, echogenic appearance that often has a swirling or ‘smoky’ appearance indicative of movement within the abdomen, secondary to respiration or active haemorrhage (Figure 2) (Arnold et al, 2008). Depth of fluid depends on the degree and duration of haemorrhage, and in some cases a haematoma may already be forming and visible within the ventral abdomen. Broad ligament and intramural haematomas can usually be visualised by placing the ultrasound probe as caudal as possible lateral to the udder in the inguinal region and have the appearance of a hyperechoic to cavitated structure (Figure 3). With haemorrhage into the broad ligament, transrectal palpation will identify a large swelling within this structure; however, this is not recommended because there are significant risks, as well as an often violent pain response associated with palpation (Crabtree, 2012). Abdominocentesis with peritoneal fluid cytology in cases of periparturient haemorrhage demonstrates a non-septic peritonitis with increased peritoneal packed cell volume (Offer et al, 2022). Abdominocentesis may not be indicated in every case of periparturient haemorrhage, but it is useful in cases where a uterine tear may be present concurrently.
Correct diagnosis and prompt treatment during the acute stage of periparturient haemorrhage is vital for survival. Therapy usually involves the judicious use of intravenous fluids, antimicrobials, an-ti-inflammatories, analgesia, procoagulant medications and treatment of any concurrent conditions, such as retained foetal membranes (Arnold et al, 2008). Blood and/or plasma transfusion may be indicated in more severe cases, although some believe that there may be an increased risk of neonatal isoerythrolysis in future foals out of mares given blood transfusions. A detailed discussion of indications for blood transfusion is beyond the scope of this article.
A combination of physical examination and clinicopathologic parameters should be considered to guide this decision, which is highly case-dependent. Factors that may prompt the need for blood transfusion are indications that the mare is decompensating and may include a combination of rising heart rate in the face of fluid resuscitation, continued or increasing signs of discomfort/agitation/anxiety, increasing lactate, decreasing packed cell volume and collapse. Plasma transfusion does not replace lost red blood cells but proves very useful in increasing circulating blood volume by providing increased oncotic pressure, as well as providing coagulation factors that have been lost.
Sedation should be used with caution, as mares may already be hypotensive; the administration of alpha-2 agonists or acepromazine may potentiate further hypotension and collapse. Administration of these medications is often required, but doses may need to be adjusted to account for the severity of hypotension. Outcome in cases of peri-parturient haemorrhage depends on the severity of haemorrhage, and some mares with massive blood loss will die despite the best of efforts. In less severe cases, and where haemorrhage can be controlled, prognosis is generally good if mares are diagnosed and treated quickly and aggressively (if indicated). Mares have a reasonable prognosis for future fertility (Arnold et al, 2008). How aggressively a mare needs to be treated is very case-dependent; some may only require a conservative approach, where mares that appear to be in shock and/or are deteriorating require aggressive intervention. Those with intramural or broad ligament haematomas are more likely to require a year off from rebreeding. It is important to note that some data strongly suggest that mares that have suffered periparturient haemorrhage once are at increased risk of subsequent episodes that may increase in severity (Turner, 2007).
Uterine tear
Uterine tears are reported to occur more frequently following dystocia. However, in the author's experience, they can occur just as commonly in mares that foal normally (Turner, 2007; Crabtree, 2012). Tears may be sustained when the mare strains persistently against an obstruction, when a fetal extremity pushes through the uterus or causes pressure necrosis, or iatrogenically by overly aggressive manipulations or fetotomy (Turner, 2007). The most common sites affected are the ventral and dorsal uterine body, and the tip of the pregnant horn. There are often no obvious clinical signs until significant abdominal contamination has occurred (Crabtree, 2012). Mares may not present for up to 72 hours post-foaling, especially if they have retained fetal membranes that may plug the hole in the uterus, delaying contamination of the abdomen and the development of clinical signs. Signs are those of septic peritonitis, and depend on the size of the tear and severity of contamination of the abdominal cavity (Crabtree, 2012). Mares will show signs of fever, bright red to purple mucous membranes secondary to endotoxaemia, tachycardia, inappetence, reduced gut motility, decreased milk production and abdominal pain. The degree of endotoxaemia is often variable, with some mares having mild intermittent fevers and some demonstrating fulminant endotoxaemic shock. Septic peritonitis results in ileus and mares often develop a distended stomach that requires decompression via nasogastric intubation. Mares may present acutely with signs of haemorrhagic shock if they have concurrent periparturient haemorrhage. In some of these cases, the uterine tear is missed as abdominocentesis is not performed. A uterine tear may also be suspected if an attempt is made to perform a uterine lavage and the lavage fluid cannot be retrieved or the mare becomes acutely painful during or afterwards.
Haematological and biochemical abnormalities include leukopenia, haemoconcentration and azotaemia (with leukopenia being most diagnostic) (Dolente et al, 2005; Turner, 2007). Transabdominal ultrasound examination reveals a large volume of free, cellular peritoneal fluid with thickening and oedema of the intestine floating within it. The uterus may or may not contain fluid depending on the location of the tear. Abdominocentesis will reveal evidence of septic peritonitis with the presence of an increased white blood cell count, often increased protein and intracellular bacteria (Frazer et al, 1997). If there is concurrent periparturient haemorrhage, the peritoneal fluid may look grossly like blood and may have an increased packed cell volume. Collection of fluid into a non-anti-coagulant tube can be helpful to differentiate haemoabdomen vs blood vessel contamination in the field. The fluid will clot if there is blood contamination or inadvertent aspiration of the spleen. The fluid should not clot with a haemorrhagic effusion. A smear that reveals phagocytosed erythrocytes is indicative of haemorrhage rather than contamination during sampling (Frazer, 2003a).
If considered safe to do so, palpation per rectum may aid in diagnosis as mares will often be very sensitive or painful when the uterus is palpated over the location of the tear. Palpation of the luminal uterine wall per vagina can be used to identify the exact location of the tear, although because the endometrial folds and uterine oedema are very pronounced immediately post-partum, it can sometimes be difficult to identify the tear (Turner, 2007). If the laceration is in the uterine body, it is within easy reach and more readily identifiable. Lacerations in the horns are more difficult to reach in the large post-partum uterus, although the author and colleagues have had good success with gently pulling the uterus caudally while within the lumen, which allows for palpation all the way to the tip of each horn. In fact, it is strongly recommended that any mare's uterus be palpated immediately after a dystocia, to attempt to identify any laceration early before secondary complications develop. If the laceration is very large, other abdominal organs (eg intestine and bladder) may be present in the uterine lumen, or at least readily palpable through the tear (Turner, 2007). Caution must be taken when palpating per vagina or per rectum as these mares may be very reactive and painful, and if they are haemorrhaging concurrently, there is risk of dislodging a clot.
Early diagnosis of a uterine laceration is critical to a successful outcome. With small or partial thickness tears where contamination of the abdominal cavity can be minimised, medical treatment in the form of broad-spectrum antimicrobials, anti-inflammato-ries, oxytocin and intravenous fluids has been described (Javsicas et al, 2010). However, the author has never successfully managed a case medically and always refers these mares for exploratory laparotomy when stabilised. Large lacerations will inevitably require surgical repair, as well as aggressive medical therapy post-opera-tively, including abdominal lavage via an abdominal drain placed at surgery (Fischer and Phillips, 1986; Javsicas et al, 2010). Surgical exploration also has the advantage of definitively determining the cause of peritonitis when it is uncertain, especially if peritonitis is from intestinal leakage, allowing accurate assessment of prognosis (Javsicas et al, 2010). Furthermore, the size of uterine defect that will resolve with medical therapy remains unknown (Javsicas et al, 2010). Mares may continue to reflux for several days until the inflammation associated with the peritonitis subsides, although those with reflux reportedly have a worse prognosis (Javsicas et al, 2010). Overall, prognosis is considered good (Javsicas et al, 2010), and mares can have foals in subsequent years, although adhesions are a potential complication which may affect future fertility (Turner, 2007).
Bladder rupture
Bladder rupture may occur as a consequence of increased intra-abdominal pressure in the foaling mare or because of direct trauma during parturition (Jones et al, 1996; Rodgerson et al, 1999; Frazer, 2003b). Clinical signs are often delayed, and mares tend to present at 36–72 hours post-foaling. Affected mares may be lethargic with a decreased appetite, although more commonly present with mild to moderate colic with tachycardia, tachypnoea and decreased gastrointestinal sounds (Rodgerson et al, 1999; Frazer, 2003b). Rectal palpation and temperature are usually within normal limits. It is important to note that mares may or may not continue to urinate normally depending on the location of the rupture.
Haematological and biochemical abnormalities often include a leukocytosis, haemoconcentration, hyperkalaemia, hyponatremia, hypochloraemia and azotaemia, although these abnormalities may not always be present (Rodgerson et al, 1999; Frazer, 2003b). Transabdominal ultrasound examination reveals a large quantity of echoic, cellular free fluid that is difficult to differentiate from haemoabdomen and septic peritonitis as a result of a uterine tear. Abdominocentesis yields cloudy yellow peritoneal fluid with a creatinine concentration that is at least twice that of peripheral concentration, consistent with urine. Calcium carbonate crystals may also be visualised (Jones et al, 1996; Rodgerson et al, 1999; Frazer, 2003b).
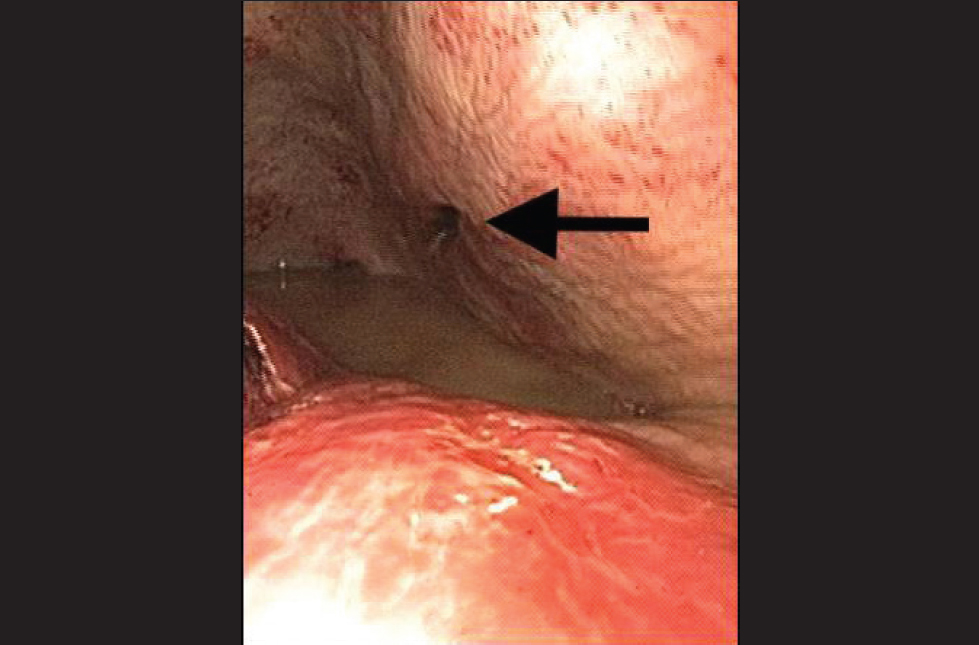
Although diagnosis can be confirmed with abdominocentesis, cystoscopy is also recommended to identify the location and size of the tear (Figure 4) for surgical planning purposes. Treatment for bladder rupture requires surgical repair of the tear and certain locations are easier to repair with the mare standing and bladder eversion (Aanes, 1988; Jones et al, 1996; Rodgerson et al, 1999).
Mares should be stabilised before surgical intervention, especially as hyperkalaemia can cause significant arrythmias with electrocardiographic abnormalities including tented T waves, widened QRS complexes and dampened P waves (Frazer, 2003b). Stabilisation involves placement of a urinary catheter and abdominal drain, as well as intravenous fluid therapy. Uroabdomen can cause a secondary chemical peritonitis and some mares may show signs of ileus, requiring nasogastric intubation. Antimicrobials and analgesia should also be instituted with caution if considering nephrotoxic medications.
Invagination of a uterine horn
Invagination of a uterine horn may occur spontaneously. However, more commonly, excessive traction on a retained fetal membrane remnant may invert the tip of the uterine horn, which may then lead to complete uterine prolapse (Perkins and Frazer, 1994). Older, multiparous mares are at increased risk likely because of repeated stretching and relaxation of the reproductive tract during pregnancy and parturition. Invaginations may also be more common following prolonged dystocia where the uterus has become atonic (Turner, 2007).
Compromised blood flow and pressure on nerve endings lead to signs of mild to moderate colic (Frazer, 2003a). Mares are often restless, persistently straining and tachycardic although some show minimal signs of discomfort. Palpation per rectum is vital for diagnosis and should include exploration of the tips of both horns. The affected horn will be shorter than normal, very thickened and a tense mesovarium may be identified (Frazer, 2003a; Crabtree, 2012). Straining following removal of retained fetal membranes may be indicative of tip inversion and should be addressed immediately to avoid uterine prolapse (Crabtree, 2012). Transabdominal and transrectal ultrasound examination reveals oedema and thickening with telescoping of concentric rings of tissue at the distal tip of the horn in question (Turner, 2007). If the invagination is not identified or not addressed quickly, then the invaginated tip can develop ischaemic necrosis (Frazer, 2003a; Crabtree, 2012). Once the nerve endings become unresponsive, mares usually become more comfortable, but they tend to relapse when secondary peritonitis ensues (Frazer, 2003a). In such cases, surgical intervention may be indicated. Abdominocentesis reveals an increased peritoneal protein concentration, although the white blood cell count tends to remain low unless there is necrosis present (Frazer et al, 1997). Reduction of the invaginated tip can be performed from within the lumen using several litres of sterile saline and manual manipulation. Repeated low doses of oxytocin (10 IU doses) helps promote uterine involution and resolution of the invagination should be confirmed by palpation per rectum (Frazer, 2003a; Crabtree, 2012). If the mare has retained fetal membranes, then they should be cut at the vulva as the weight of the membranes on the tip of the horn contributes to the invagination (Turner, 2007).
Conclusions
Post-foaling colic is generally demonstrated by non-specific signs of discomfort and can be challenging to diagnose. This article covered conditions of the genitourinary and reproductive tracts. Part 1 of this series covered some of the more commonly encountered gastrointestinal conditions. Regardless of the origin of the discomfort, the identification of some key features described in this article will aid in accurate diagnosis, which is vital to allow rapid stabilisation and appropriate treatment of these often-critical mares. EQ
Conflicts of interest The author declares that there are no conflicts of interest.